How I Fix Stubborn Medial Elbow Pain / 'Tendinitis' (PT's Full Comprehensive Protocol)
Hooper’s Beta Ep. 162
Introduction
I’ve helped countless people recover from medial elbow pain in my practice and today I’m going to give all of that knowledge to you… or at least the most relevant parts. In this video you’ll learn everything you need to know about elbow pain in and around the medial epicondyle – commonly known as climber’s or golfer’s elbow – including what causes it, what to do to fix it, and how long it takes to get back to 100%. We’ll even add a bit of secret sauce that could be the key to unlocking your recovery.
Disclaimer
All this information is for educational purposes only. None of it should be taken as medical advice or a replacement for seeing a qualified professional. Certain injuries such as ligament tears, elbow dislocations, snapping elbow syndrome, and bone fractures will not be covered here. Proceed at your own risk.
What causes medial elbow pain?
There are two common causes of medial elbow pain that we’ll focus on: tendon pathologies (tendonitis / tendinopathies) and nerve compression or impingement.
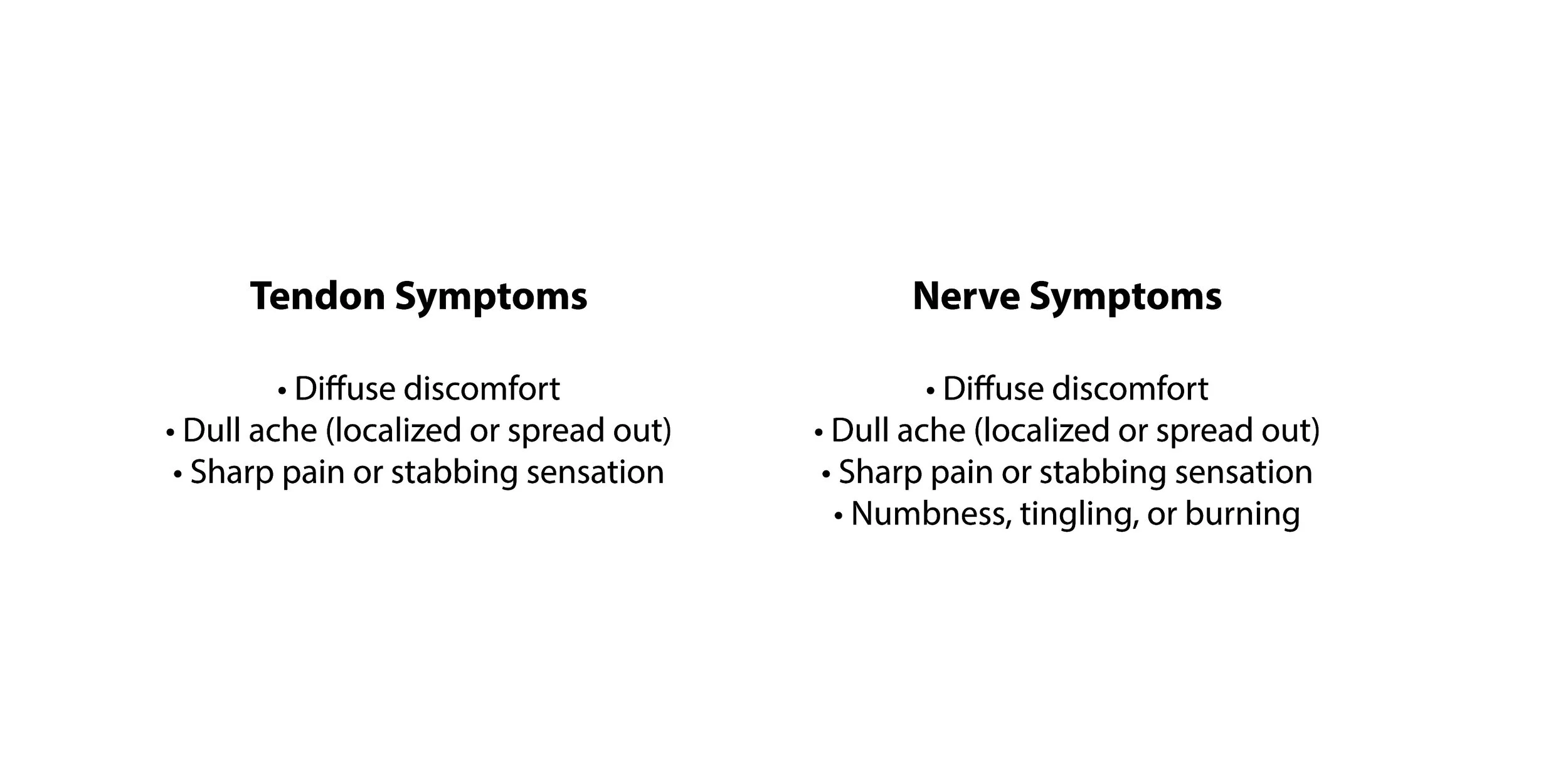
Tendon pathologies are the ones most people are familiar with, causing diffuse discomfort in the elbow, a dull ache (which may be localized or spread out), and/or a sharp or stabbing sensation. This issue usually occurs from what we call “overuse,” which is a chronic build up of tissue damage. If you’re not familiar, this process happens because performing novel, intense, or repetitive activities, like resistance training, hard climbing, or swinging a golf club, can cause a small amount of damage to our soft tissues, including tendons. This is not necessarily a bad thing; in fact, it’s an important byproduct of training that signals our bodies to adapt and improve those tissues so, next time we perform that activity, we’re better equipped to handle it. However, those adaptations take time, and sometimes they haven’t finished by the time we’re back at the gym or golf course. We may *feel* like we’re fully recovered, especially because our muscles tend to adapt much quicker than tendons, but that doesn’t mean all the tissues are back to 100%. Thus, a little bit more damage occurs to the tendons before they’ve had time to fully heal. Again, this usually isn’t an issue in the short term. However, when this occurs over and over again, the slow build-up of damage to the tendon eventually becomes significant enough to make itself known as pain. So, medial elbow pain that’s caused by overuse is a result of certain tendons being constantly asked to perform more work than they can recover from. Specifically, the most commonly involved tendons are those of the flexor carpi ulnaris (FCU), pronator teres (PT), and flexor digitorum superficialis (FDS).
Nerve-related pain, on the other hand, is a different beast. It’s actually the one that constantly gets overlooked, which is partly why so many people feel like they can’t get rid of their elbow pain. In fact, I even helped write a paper on this! Why is everyone making this mistake? Because most people think nerve symptoms can only be a tingling or burning sensation, but that’s not actually true. The real symptoms of nerve compression are: diffuse discomfort, a dull ache (which may be localized or spread out), a sharp or stabbing sensation, and/or numbness, tingling, or burning. Sounds familiar, right? Turns out nerve symptoms in the elbow can mimic the symptoms of a tendon pathology, so if you have any of those overlapping symptoms you shouldn’t immediately assume it’s a tendon issue. Nerves are unsurprisingly quite sensitive, so when one gets compressed too much by a muscle, it tends to let you know. Compression of the ulnar nerve at the elbow is called cubital tunnel syndrome (CTS), while compression of the median nerve at the elbow is called pronator teres syndrome (PTS). Since the ulnar and median nerves pass through, under, and between muscles in our elbows and forearms, you can imagine how frequent gripping or pullup-like movements could squeeze them.
Now, with so much overlap between tendon and nerve symptoms, you might be wondering how you can tell which one is actually causing your elbow pain…
How do I know if my symptoms are tendon or nerve?
This can be quite tricky to figure out, because the activities that provoke your symptoms could be irritating either the tendon or the nerve… or both. For example, when you do a pullup, you’re putting strain on those elbow tendons, but the muscle contraction can also squeeze the nerves. However, there are some useful indicators to look for.
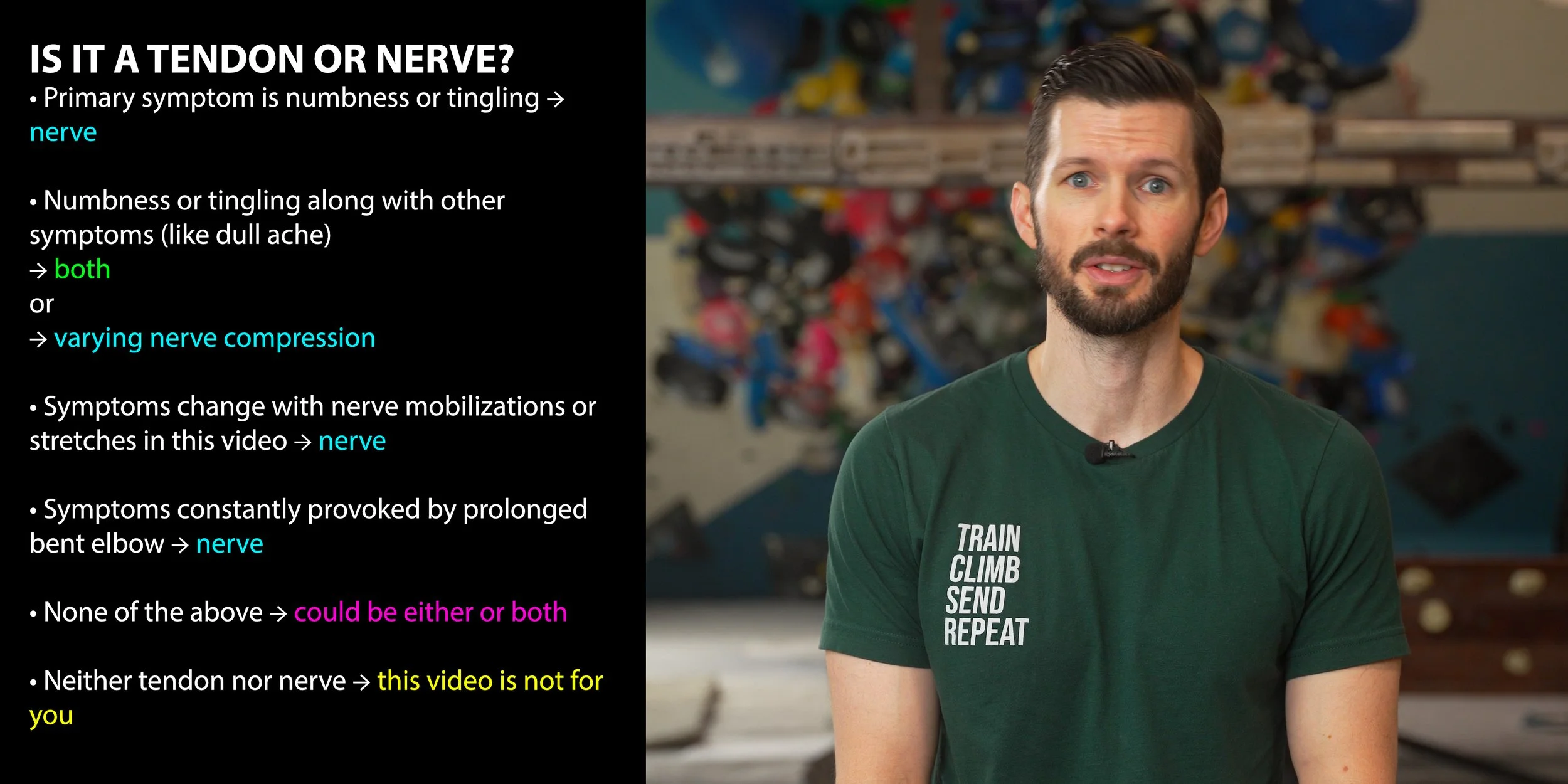
Numbness and tingling are symptoms only associated with nerve compression. If you experience this as your primary symptom, it is a nerve.
If you have numbness or tingling along with other symptoms like a dull ache, you might have a combination of nerve and tendon involvement, or you might simply have varying levels of nerve compression at different times. For example, you might sometimes have mild compression that causes a dull ache and other times have more significant compression that causes numbness or tingling. So, combination symptoms could be tendon and nerve or just nerve.
If your symptoms change with the nerve mobilizations or the stretches I’ll be showing you for the chest/shoulder, a nerve is involved.
If your symptoms are constantly provoked when your elbow is bent, such as holding your phone for too long, a nerve is likely involved.

If you’re positive that your symptoms are *only* nerve related, then you should watch our video “How to Fix Nerve Tension for Climbers” instead of this one. If you think your symptoms are related to *neither* tendons nor nerves (such as an ulnar collateral ligament sprain, osteochondral dissecans, arthritis, snapping elbow syndrome, or any other ligament or bone issue), this video is unfortunately not for you.
For everyone else, I recommend you complete the routine we’re about to lay out even if you’re dubious about nerve involvement. Since it is possible for medial elbow pain to be caused by *both* a tendon and a nerve issue, the secret sauce we mentioned earlier turns out to be treating *both* issues. It's hard for most non-professionals to properly assess their own nerve issues, so it’s worth performing the nerve exercises for at least a couple weeks. It won't cost you that much extra time and you could very well be surprised by the results.
How Do I Recover?
About This Protocol
Before you begin this protocol, you should have a bit of context. Because there are multiple structures that can cause symptoms at the elbow, the exact recovery exercises needed can vary from one person to the next. That means a few things:
For the best chance of success, this program will take a broad, cover-all-the-bases approach. While this method has proven quite effective in lieu of an individually-tailer program, it does mean the protocol involves a lot of exercises. But don’t let that discourage you; it won’t take long to get the hang of it.
We’re not going to cover every single regression and progression of each exercise because this video would never end. If what we lay out here is too hard for your current stage of recovery, you’ll need to regress the difficulty to the appropriate level on your own. Of course, if you don’t want to deal with that, remember you can always use one of our pre-made Recovery Blueprints to make it extremely easy.
This is not a personalized program, so you may find there are exercises here *you* don’t need but that may be extremely beneficial for someone else.
You will need access to some tools, namely dumbbells (or a cable machine), a lever bar or hammer (or better yet our Torque devices), and resistance bands.
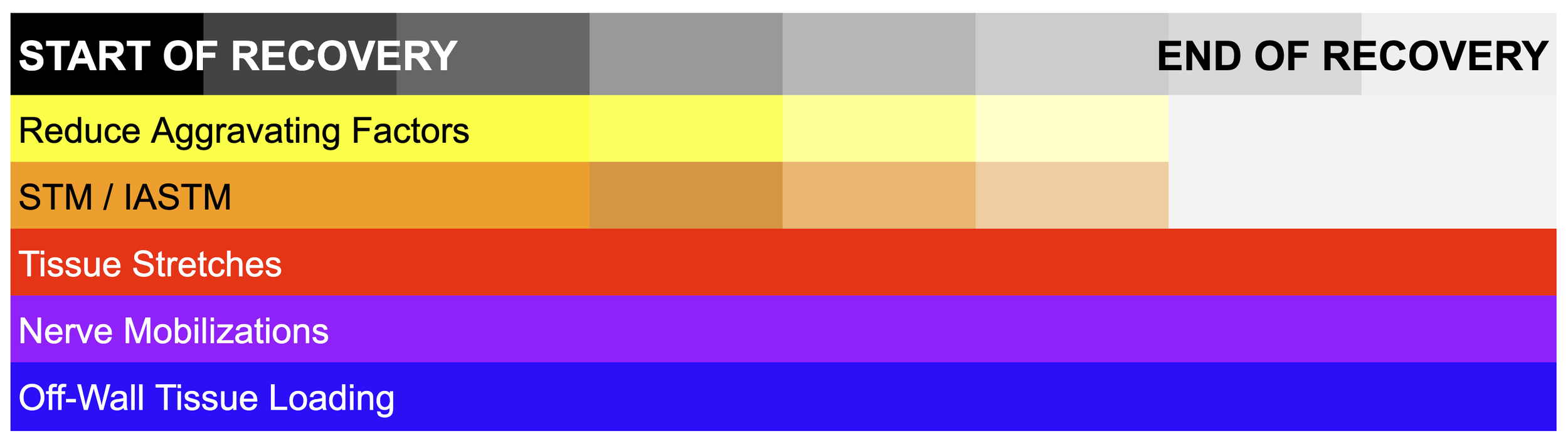
1. Reduce Aggravating Factors
The first step toward recovery is the one no one wants to hear because it’s boring and stupidly obvious, but that’s exactly why so many people make the mistake of overlooking it. So don’t be one of those people! You need to reduce aggravating factors, which are things that make your symptoms worse. As mentioned, often one of the causes of elbow pain is simply too much work being asked of specific tissues, so you can’t expect to recover if you keep piling on the same work.
This does *not* mean you should stop *all* activity; but you need to cut back on the aggravating factors based on the severity of your symptoms. In general, if the pain from an activity does not exceed 2/10 *during* and *24 hours after* you do it, that activity is likely fine. If an activity causes more or longer-lasting pain than that, you likely need to reduce the intensity, reduce the volume, or change the movement style to bring the pain down to the acceptable level.
2. Soft Tissue Mobilization (STM) / Instrument Assisted Soft Tissue Mobilization (IASTM)
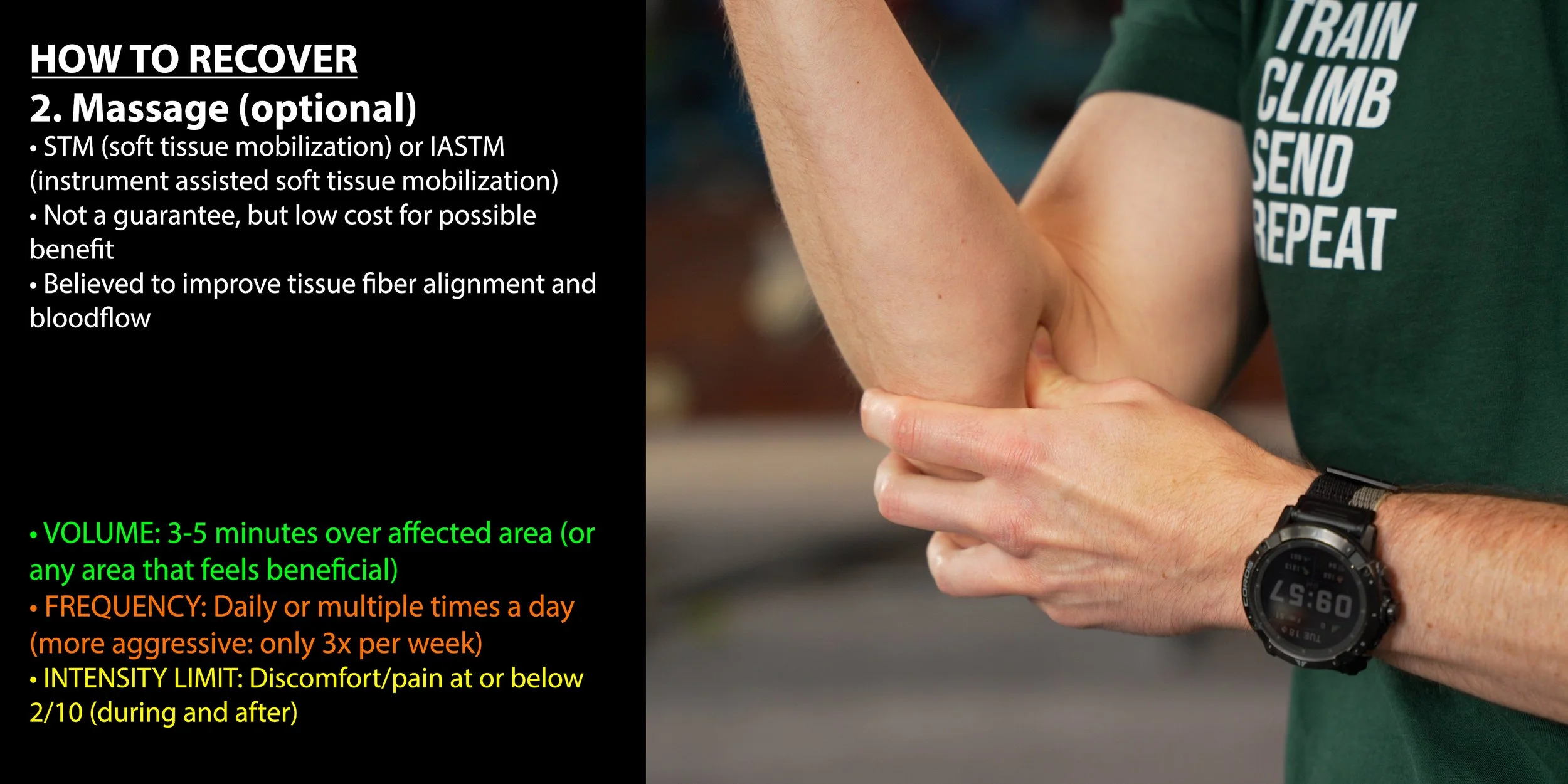
STM and IASTM are both forms of massage therapy, which is a low cost method that could have a positive impact on your healing. It’s not a guarantee, but it’s thought to improve the alignment of new tissue, increase blood flow to the area, and increase neurological awareness of the area. Note: it is optional here. If you find that it irritates or worsens your symptoms, it might be because the painful structure you’re trying to massage is actually your nerve, and it might not like that. So if this type of massage makes things worse or does nothing for you, discontinue it.
Frequency and Duration
Perform for 3-5 minutes over the affected area (or any area that feels beneficial). This can be done daily or multiple times a day if you’re using gentle pressure. IASTM with more aggressive pressure should be limited to roughly three times per week.
3. Tissue Stretches
Next, let’s get into a few different stretches. Unlike the optional massaging, I do recommend you perform these stretches even if you don’t notice an immediate change in your symptoms. It may take a couple weeks for the benefits to show up.
1: Flexor Stretch + Nerve Glide

Up first is a combination stretch to loosen tight forearm muscles while mobilizing the ulnar and median nerves.
HOW TO:
1. Start with the target hand directly in front of you, palm facing down, fingers straight and extended, and elbow gently bent.
2. Use your other hand to gently pull your fingers and wrist upward (into extension) until you feel a comfortable stretch in your elbow, forearm, and/or hand.
3. While maintaining this stretch, slowly straighten your elbow as much as you can without discomfort. You will likely feel the stretch increase. If needed, release some pressure on your fingers to adjust the intensity. If you can completely straighten your elbow, great! Hold for approximately 3-5 seconds, then return to the gently bent position.
4. Next, while maintaining the stretch in your fingers and wrist, bend your elbow to allow it to fully flex. If you feel discomfort due to too much elbow bending, ease off the elbow flex or reduce the pressure on your fingers. Hold for 3-5 seconds.
5. Move back and forth between the bent and straight elbow positions.
Sets/Reps/Frequency/Hold TIme
This stretch can be performed multiple times per day. You should perform 2-3 sets with 3-5 reps. One rep is counted as one time with the elbow straight and one time flexed (so three repetitions would mean three times with the elbow straight and three with the elbow bent). Hold each position for 2-5 seconds.
2: Pec 90 & 120 stretches
Up next will be two pec stretches: one with the arm at 90 degrees to add a rotational component to the stretch, and the other at about 120 degrees to get more pec minor involvement.
These two stretches are important because elbow pain can stem from nerve tension as a result of compression in the chest or shoulder region. Performing pec stretches can mobilize these areas and help alleviate this compression, leading to reduced elbow discomfort.
To perform the Pec 90 stretch:
Stand with your feet staggered. I recommend placing your left foot forward if stretching your right arm.
Place your hand on the doorframe (or sturdy surface). Your arm should be raised 90 degrees to the side (elbow at shoulder height) and your forearm should be vertical (elbow bent to 90 degrees). Your palm should be facing forward.
To begin the stretch, take a small step forward until you feel a gentle stretch in the chest or shoulder.
At the same time, slightly angle your chest down toward the ground and away from the arm that is on the doorframe to improve the stretch.
Hold this position for 20-30 seconds, then switch sides and perform with the other arm.
To perform the Pec 120 stretch:
Stand with your feet staggered. I recommend placing your left foot forward if stretching your right arm.
Place your hand on the doorframe (or sturdy surface) above head height. Your palm should face forward and your elbow should be gently bent.
To begin the stretch, take a small step forward until you feel a gentle stretch in the chest or shoulder.
At the same time, slightly angle your chest down towards the ground and away from the arm that is on the doorframe to improve the stretch.
Hold this position for 20-30 seconds, then switch sides and perform with the other arm.
Sets/Reps/Frequency/Hold Time
These stretches can all be performed multiple times a day. Perform one set of 2-3 reps. Hold each rep for 20-30 seconds.
Notes
During these stretches, you should avoid engaging your midback to try and enhance the stretch; your midback should be relaxed.
If you feel any numbness or tingling in your target arm, you should stop the stretch and return the arm to your side until normal sensation is restored. Once that is achieved you can perform the stretch again.
Staggering your feet is important so you aren’t holding yourself up with your arm, which would reduce the effectiveness of this stretch.
You can vary the amount of forward lean or rotation (or combination thereof), to find what feels best to you.
Determining Intensity for These Stretches
These stretches should not be painful. Apply only enough force to generate a mild stretch. While a small amount of discomfort (1-2/10) may be experienced, it should never truly feel painful. If you do start to feel pain, reduce the stretch intensity by reducing the range of motion or the amount of force you’re using.
4. Isolated Nerve Mobilizations
Let’s now get into some isolated nerve mobilizations. There are two primary techniques: nerve flossing, which is the gentlest form, and nerve tensioning, which is the most aggressive form. To be efficient and not make this video two hours long, we’re not going to perform those two techniques, but rather we’ll add a bit more secret sauce and show you the ultra-efficient “nerve floss + tension” hybrid technique. Just note: if you find this hybrid technique to be too aggressive, you should regress to the nerve flossing techniques discussed immediately below.
Hands-low median nerve floss
To perform the hands-low median nerve floss:
Start in a standing position looking straight ahead, with your target arm’s elbow fully bent, hand in a gentle fist facing in towards your bicep/shoulder.
Straighten your elbow while uncurling your fingers. Extend your wrist backward and allow your shoulder to gently extend behind your body. Your fingers should be pointing straight backward. You should finish in a position where it is like you are trying to place your palm on the ground behind you.
While the elbow is straightening, simultaneously rotate or lean your head in the same direction (if straightening the right arm, move your head to the right. This decreases tension on the nerve).
Hold for 1 second or less then return to the starting position with your elbow flexed and once again looking straight ahead.
You have now completed 1 repetition. Repeat as indicated in your app.
Hands-high median nerve floss
To perform the hands-high median nerve floss:
Start in a standing position looking straight ahead, with your target arm raised directly out to the side, elbow fully bent, hand in a gentle fist and wrist relaxed.
Straighten your elbow while uncurling your fingers. Extend your wrist backward while pointing your fingers upward. Your fingers should be pointing up toward the sky at the end of the movement.
While the elbow is straightening, simultaneously rotate or lean your head in the same direction (if straightening the right arm, move your head to the right. This decreases tension on the nerve).
Hold for 1 second or less then return to the starting position with your elbow flexed and once again looking straight ahead.
You have now completed 1 repetition. Repeat as indicated in your app.
Ulnar nerve flossing
To perform ulnar nerve flossing:
Start in a standing position looking straight ahead, with your arm raised directly out to the side, elbow straight and hand relaxed.
Bend your elbow while extending your hand and fingers back, as if trying to point in towards your head.
While the elbow is bending, simultaneously rotate or lean your head in the same direction (if straightening the right arm, move your head to the right. This decreases tension on the nerve).
Hold for 1 second or less then return to the starting position with your elbow flexed and once again looking straight ahead.
You have now completed 1 repetition. Repeat as indicated in your app.
Determining Intensity
Nerve *flossing* should not produce pain or discomfort. If done correctly, minimal to no tension is placed on the nerve, so there should not be a strong stretching sensation (a mild stretch is OK). The absence of sensation does not mean it's ineffective.
Sets/Reps/Frequency
Because nerve flossing is a gentle activity, it can be performed multiple times a day. Individual response will vary though and it is recommended to start with a lower frequency (such as 1x/day) when it is new to you. Perform 1-2 sets of 6 repetitions for each nerve flossing technique. This activity can be done daily.
1. Hands-Low Median Nerve Floss + Tension
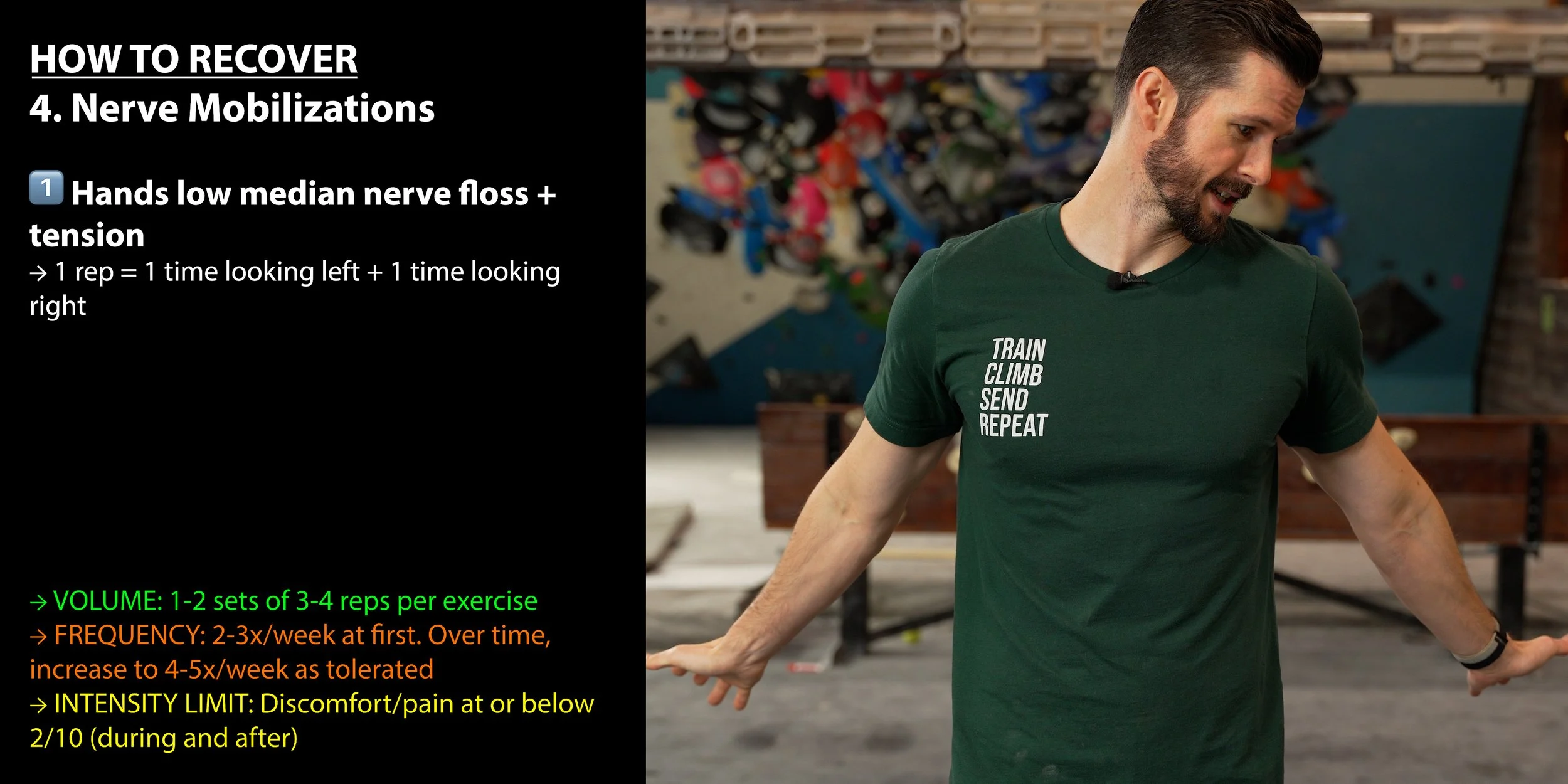
To perform hands-low median nerve floss + tension
Start with both elbows fully bent and hands in fists, palms facing your shoulders. You should be looking straight ahead.
Straighten both elbows and open up your hands, extending your fingers and wrists. Do not rotate your arms. At the bottom of the movement, your biceps and forearms should still be pointing forward. Keep your shoulders down (do not allow them to shrug up) and extend your arms slightly behind your body. Extend your wrists as if trying to place your palms on the ground behind you.
While moving your arms, simultaneously turn your head to look at one of your hands (e.g., turn your head down and to the left as your arms extend).
Return to the starting position.
Repeat the arm movement, but this time, turn your head to look at the opposite hand (e.g., turn your head to the right).
Return to the starting position. You have now completed one rep.
2. Hands-High Median Nerve Floss + Tension

To perform hands-high Median Nerve Floss + Tension
Start with your hands at eye-level, elbows bent to 90 degrees, and wrists flexed (but relaxed).
Straighten both arms simultaneously, while extending the wrists and fingers up toward the sky.
While moving your arms, simultaneously turn your head to look at one of your hands (e.g., turn your head to the left as your arms extend).
Return to the starting position.
Repeat the arm movement, but this time, turn your head to look at the opposite hand (e.g., turn your head to the right).
Return to the starting position. You have now completed one rep.
3. Ulnar Nerve Floss + Tension w/ Levels
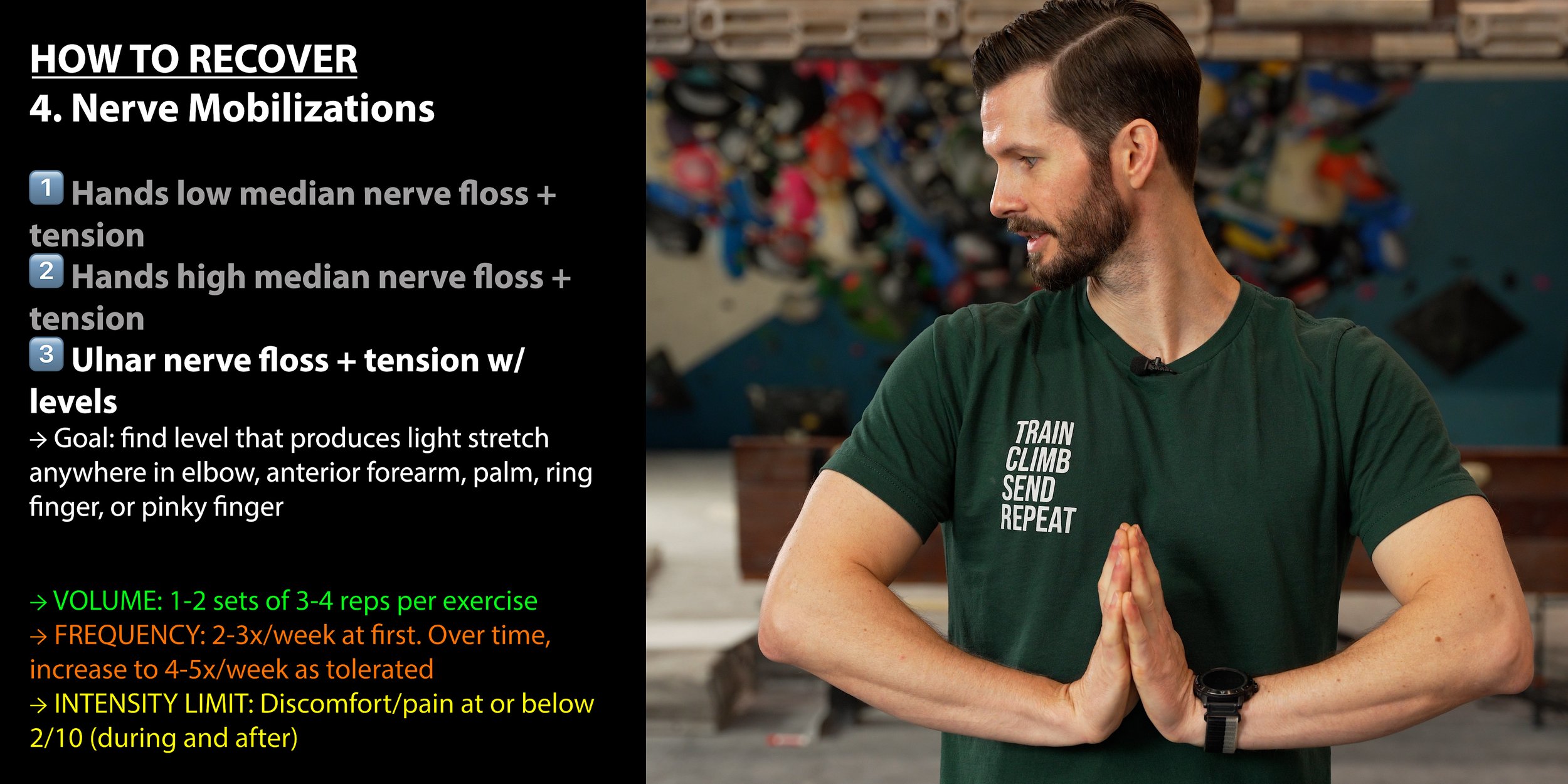
Our final nerve movement will involve the ulnar nerve with different levels of intensity. The goal is to find a level that produces a light stretching sensation anywhere in the elbow, anterior forearm, palm, ring finger, or pinky finger. If you feel any numbness or sharp tingling, immediately reduce the range of motion or stop the exercise until symptoms subside.
LEVEL 1️⃣: Lightly press your hands together in a "prayer" position (palms together, fingers pointing upward) at chest level. Slowly lower your hands downward, keeping the palms pressed together (be sure to keep pressure in the ring and pinky fingers) Stop when you feel a stretch along the inner side of your forearms, wrists, or hands (particularly the pinky or ring fingers). Hold for 2-5 seconds then move in and out of this position.
LEVEL 2️⃣: Same as level 1, but with a simple rotation or lateral lean of your head from side to side. Hold each side for 2-5 seconds.
LEVEL 3️⃣: Get into the prayer stretch position, then slide your hands left and right while looking straight ahead. Make sure that your hands stay low. Don’t allow them to move up towards your armpit as you slide side to side. Hold each position for 2-5 seconds.
LEVEL 4️⃣: Combine levels 2 and 3, moving your head away from the side that your hands are moving toward. Hold for 2-5 seconds in each position. Rest after 3 reps on each side.
Determining Intensity
With nerve floss + tension techniques, there should be a gentle stretch in one arm at a time but it should not cause pain or discomfort. Some symptoms may temporarily increase for up to a few minutes but should not last longer than that. If you feel pain or discomfort, check your form. If you believe you are doing this correctly and still experience an excessive increase in symptoms, try reducing the range of motion to reduce the intensity. If that doesn’t work, discontinue this activity and consider seeking out more in-depth management of this issue with a qualified healthcare provider. You may have some nerve tension contributing to your symptoms that requires additional management.
Sets/Reps/Frequency
Perform 1-2 sets of 3-4 reps for each mobilization.. Since this technique does involve nerve tensioning, it should be performed at most 2-3 times per week for most individuals initially. Over time, if you notice it’s beneficial you can increase to up to 4-5 times per week as tolerated.
5. Off-The-Wall Tissue Loading
Finally, we’ll need to do some off-the-wall tissue strengthening. Of course, you might be asking: “Why are you telling us to add these exercises when earlier you said a primary cause of this issue is doing too much?” Great question!
First, we don’t ever want to completely eliminate *all* loads. A complete absence of stimulus is *not* a faster recovery. Your tissues heal better and faster when controlled, specific, well-programmed loads are applied to them. These exercises do just that while strengthening the surrounding muscles as a bonus.
It’s easier to program loads when they are done off the wall, where you can easily adjust the reps, sets, and weights. Compare this to climbing or other sports where you can’t effectively moderate and track the load on your elbows.
Compared to climbing, off-the-wall training is better for targeting specific muscles or muscle groups to strengthen. Rather than guessing how much work your flexor carpi ulnaris is doing, you can specifically load it off the wall and increase its work capacity in a measured way.
Replacing aggravating factors with specific recovery exercises gives you a controlled environment to better understand your symptoms and how they respond to certain exercises.
Phew! That’s it! We now have our basis covered.
Superset 1: Forearm Pronation and Wrist Flexion
To start things off, we’ll do forearm pronation followed by wrist flexion.
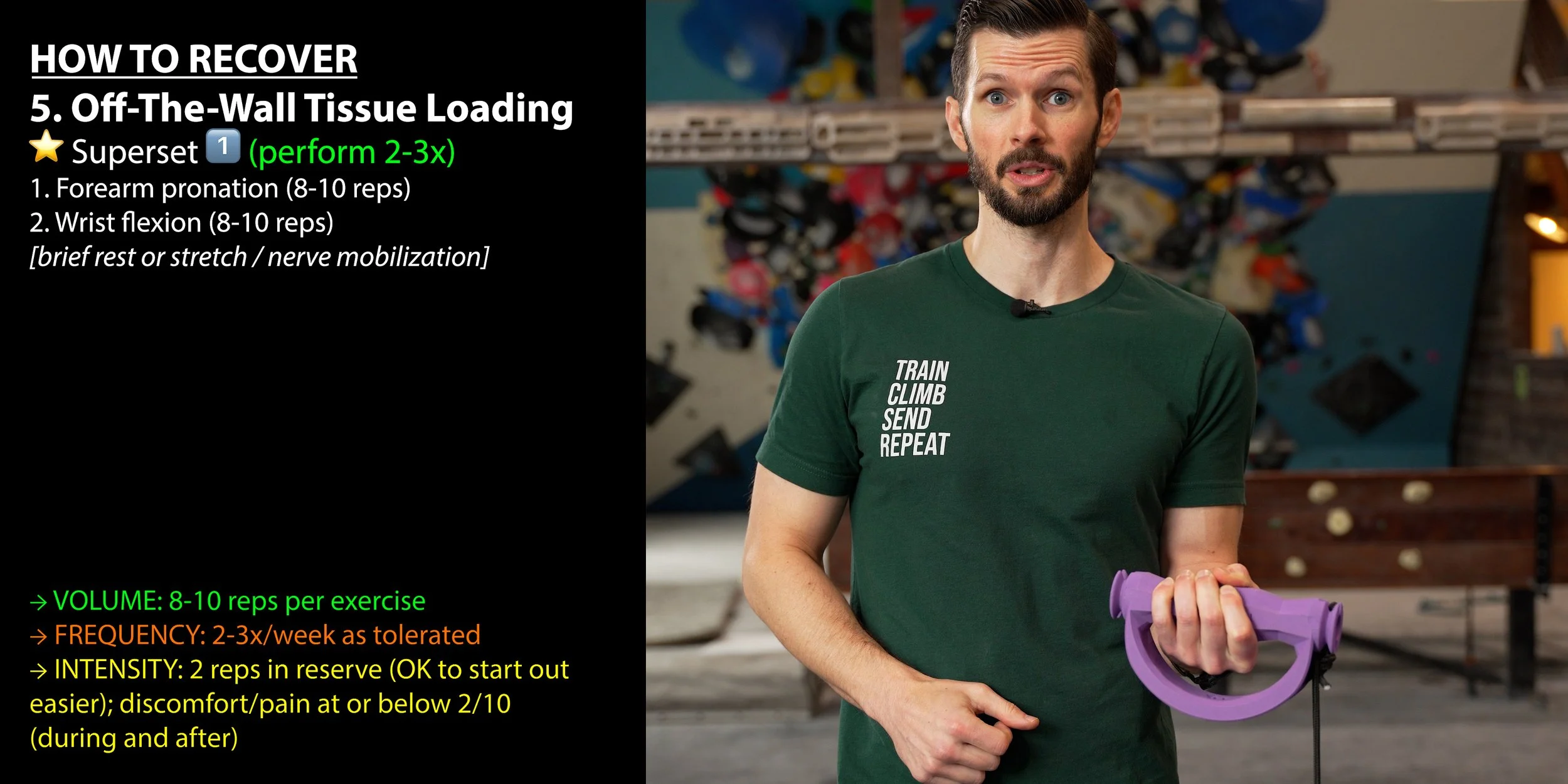
Purpose
Forearm pronation specifically targets the pronator teres muscle which attaches to the medial epicondyle.
Wrist flexion helps to isolate the wrist flexor FCU which attaches to the medial epicondyle.
To perform forearm pronation:

ADJUSTABLE DUMBBELLS OR LEVER BAR: Add weight to one side while leaving the other empty or at a lower weight (for example, 5 pounds on one side and 10 pounds on the other). Grab it at its normal grip point, but hold it so the heavier side (10 pounds in this example) is on top.
NON-ADJUSTABLE DUMBBELLS: Grab the dumbbell on one end (the actual weight, not the handle) and hold it vertically so the other end points toward the ceiling.
HAMMER: Grab the hammer by the handle and hold it vertically with the metal head up towards the sky.
To perform wrist flexion:

Hold a dumbbell with a thumb-over grip (thumb on the same side as your fingers).
Rest your forearm on a bench or table (or even your leg) with your elbow bent to about 90 degrees and your palm towards the ceiling (wrist in a straight/neutral position).
While keeping the dumbbell horizontal and your forearm flat on the surface (avoid lifting off), lower the weight towards the ground by allowing your wrist to flex, moving through all available range of motion.
Pause momentarily at the bottom of the movement, then lift the weight back up as high as you comfortably can.
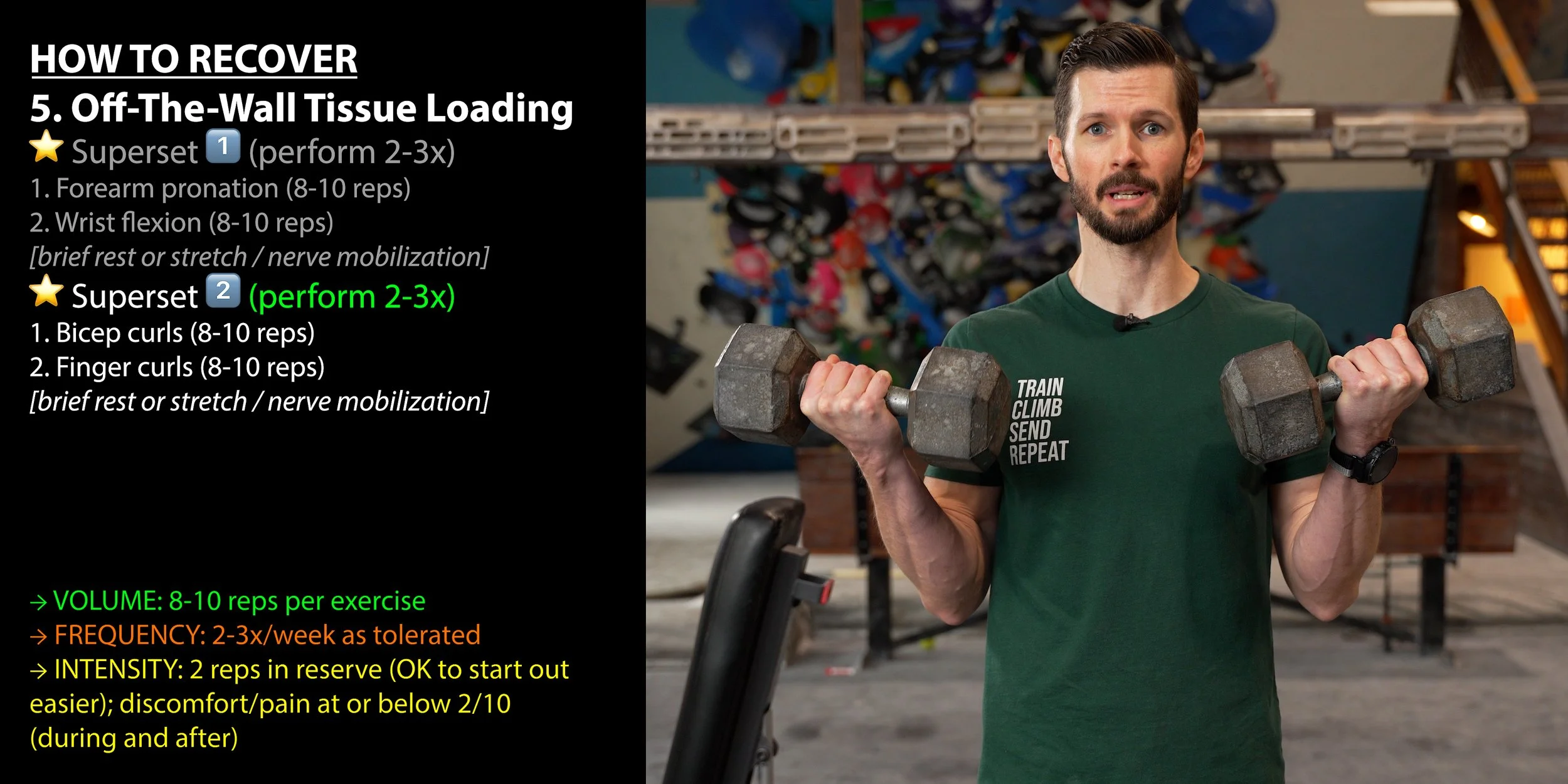
Superset 2: Bicep Curls and Finger Curls
For superset two, we’ll start with bicep curls and finish with finger curls.
Bicep curls help train the bicep brachii and the brachialis muscles which may contribute to medial elbow pain.
Finger Curls specifically target the FDS and FDP isotonically. The FDS attaches to the medial epicondyle while the FDP attaches near the medial elbow which may contribute to pain.
To perform bicep curls:
Adjust the cable system so it’s anchored below you and there’s tension on the system with your arms fully extended by your side (or, if using dumbbells, simply hold one in each hand by your side).
Hold the handles with thumb-side facing forward, then flex your right elbow, bringing the handle up as high as you can while also rotating it so your palm ends up facing your shoulder. Try to mostly isolate the elbow movement here rather than assisting it by arching your back or flexing your shoulder.
Lower the weight back down with control (reversing the rotation as you do), then perform the next rep on the left arm.
You’ve now completed one rep (left + right = one rep).
To perform finger curls:
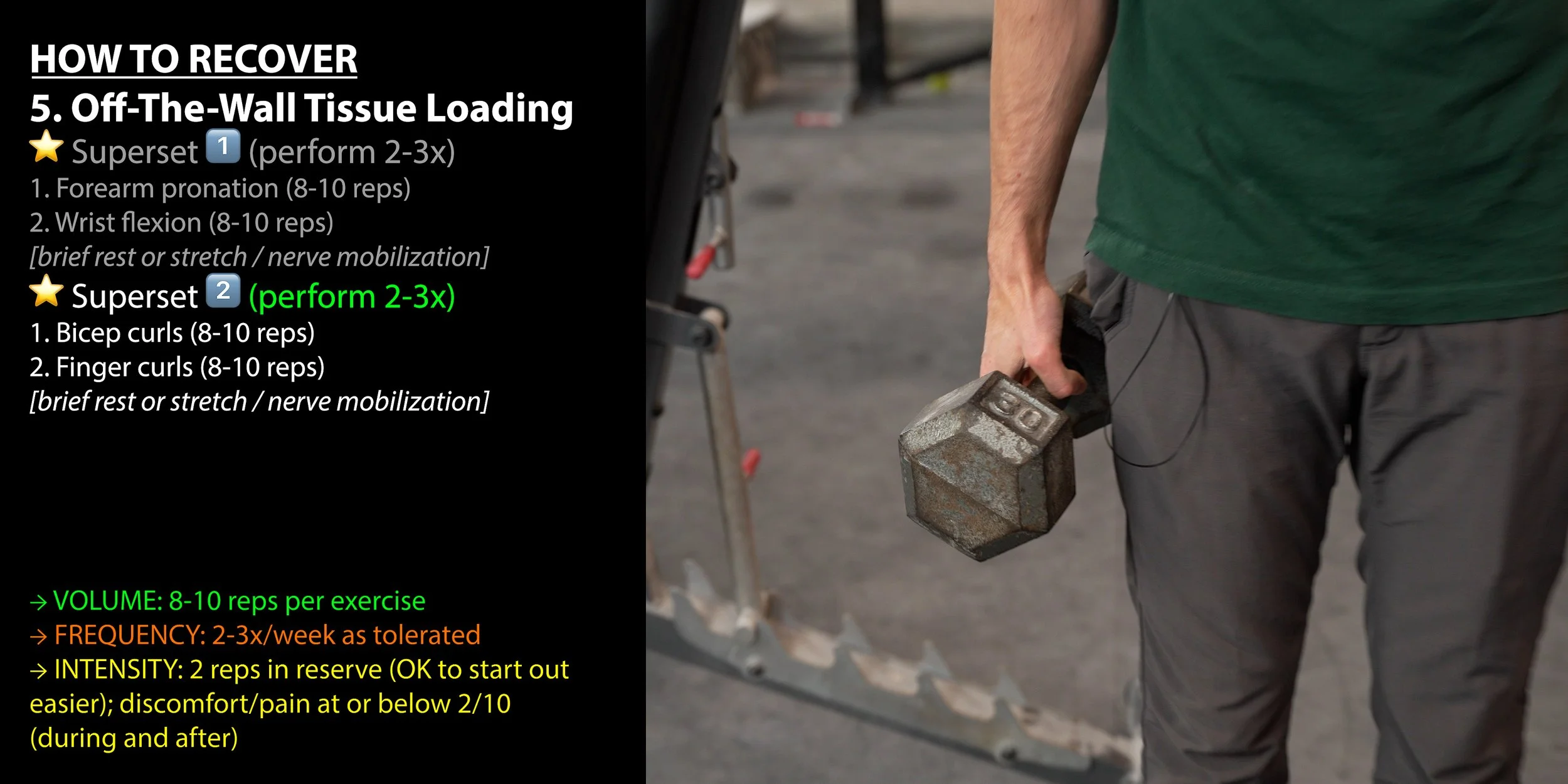
Hold a dumbbell in each hand at your side, arms relaxed.
Relax your fingers to allow the weight to roll down towards your finger tips, but be careful not to drop the weight.
Pause at the bottom of the movement, then curl the weights back to the starting positions.
And that’s it for this routine! But let’s get into some useful programming notes:
Optional Rest/Stretch
After each set of the superset, you can take a short break or you can add in one of the tissue stretches or nerve mobilization techniques while you recover. Using Superset 1 for example: perform 8 reps of rows, 8 reps of forearm supination, and then perform the pec 90 stretch before repeating that superset.
How much weight should I be using for all these exercises?
You should use enough weight to achieve an intensity of about 2 RIR (reps in reserve) as long as you’re not causing more than 2/10 pain or completely sacrificing form. When you’re new to this, start with a lower intensity to get acquainted with the movements and then work up.
How many supersets should I do?
If this routine is new to you, I recommend only performing each superset twice per session, that way you don’t add a ton of load right off the bat. Once you know you can tolerate that, add a third round. Perform each superset in the order we presented here, completing all rounds of one superset before moving on to the next (e.g. superset one x2, superset two x2).
How often should I be doing this routine?
2-3x/week as tolerated.
How Long Will It Take to Recover?
If it turns out that it was just your pesky nerves causing the issue the entire time, you should notice a quick improvement in symptoms, within a few days to a few weeks. Though, keep in mind you might have to manage this long term and some nerve symptoms can take much longer to fully resolve. If you notice an improvement with the nerve techniques and stretches, keep them up!
If it’s a regular ole tendon pathology, it can take 2-4 months to recover depending on how severe it was initially and how well you program your recovery.
Alternative Forms of Treatment





If you are struggling with elbow pain that doesn’t respond to load management, strength training, or nerve mobilizations, the first step would be to seek professional medical advice for individualized treatment. But here are a few other options that you should be aware of:
Injections, including cortisone, PRP, and prolotherapy among others
Extracorporeal shockwave therapy, which is a non-invasive treatment that delivers high-energy acoustic waves to the painful tendon area
Dry needling, which involves inserting thin, sterile needles into specific myofascial trigger points (muscle knots) in the tight forearm muscles
Bracing, which can help if you’re experiencing symptoms from your elbow being in a certain position while you sleep.
Ice, which can help some individuals immediately after activity to calm a reactive tendon or nerve
Heat, which can relax tight muscles and promote blood flow
The Most Convenient Way to Recover

Remember if you want to take the guesswork out of your recovery, save yourself a whole lot of time, and get a program that’s specifically designed for recovering from medial elbow pain, which combines stretches, nerve mobility, and strength training all into one convenient routine on your phone, you can get that today on our website at hoopersbeta.com/recoveryblueprint. These are the exact injury-specific programs I’ve used in my practice to help hundreds of climbers get back on the wall pain-free. They’ll take you from the earliest stages of healing all the way to regaining full strength and returning to peak performance. Our Recovery Blueprints are a proven way to fast-track your recovery and get you climbing hard again. We don’t just have elbow recovery blueprints either! If you’ve been dealing with Finger or TFCC pain, we’ve got you covered, with more to come in the future!
Can I Do Anything to Avoid Medial Elbow Pain?
Last but not least, here are a few strategies to help reduce risk.
1. Manage Your Load
Load management is the key to progress in so many realms, but it’s also the key to avoiding most tendinopathies. So make sure you aren’t constantly exceeding your tendon’s ability to recover from the training you're placing on it by not ignoring pain, making sure to treat recovery as a part of your training, and remembering that just because climbing kids might do 6 hour sessions 5x/week, doesn’t mean you can. If you do all that, you can avoid most elbow pain.
2. Expose Yourself
Keep those muscles strong! Sometimes on-the-wall training isn’t enough, so train those elbows up! The exercises in this routine will help with loads of movements on the wall and will make your muscles and tendons more resilient over time.
If you’re interested in reading that research paper I mentioned but don’t have access, just email pt@hoopersbeta.com - until next time: train, climb, send, repeat!
DISCLAIMER
The Beta Agency is providing content on its website that aims to inform rock climbing enthusiasts and/or individuals interested in the field of physical therapy of the various physical conditions that may befall those engaged in the sport of rock climbing, for informational purposes only. None of the information provided by The Beta Agency should be regarded as medical advice or construed to be a medical diagnosis of any form. By using our products, services, and/or the information on our website, you acknowledge that you understand this information is not meant to be a substitute for medical advice from an appropriate licensed healthcare professional, and that you will not rely on any of the information you acquire from us as the sole basis, personally or as a suggestion to others, to make any healthcare-related decision(s). If you suspect that you may have a medical condition that you are trying to diagnose, we strongly urge you to seek the advice of an appropriate medical practitioner. If you have a medical emergency, you should contact emergency services immediately.
Click for full Terms and Conditions and Privacy Policy