This Common Finger Pain is NOT a Pulley Injury (HOW TO FIX IT)
Hooper’s Beta Ep. 118
INTRODUCTION
At this point I think most climbers are aware of the pulleys in our fingers, and some are all too familiar with the pain they can cause when they get injured. Oddly enough, however, many climbers experiencing pain at their pulleys may not have a pulley injury at all! There is actually a completely different injury that presents with many of the same symptoms. It’s called flexor tenosynovitis and as the name implies it involves the finger flexors that run underneath the pulleys. With so many similarities it can be tricky to differentiate between this tenosynovitis and a pulley injury, so in this video we’re going to show you how to figure out which issue you really have and how the treatment differs between them. We’ll also use this handy little ultrasound so we can see in real time what flexor tenosynovitis actually looks like. And who knows, maybe you’ll find out your pulleys are actually perfectly fine!

WHAT IS IT?
So what is finger flexor tenosynovitis? You might think it’s some sort of irritation of the tendon itself, but it’s actually inflammation of the sheath that surrounds it, caused by friction between the sheath and the pulleys when under heavy load.


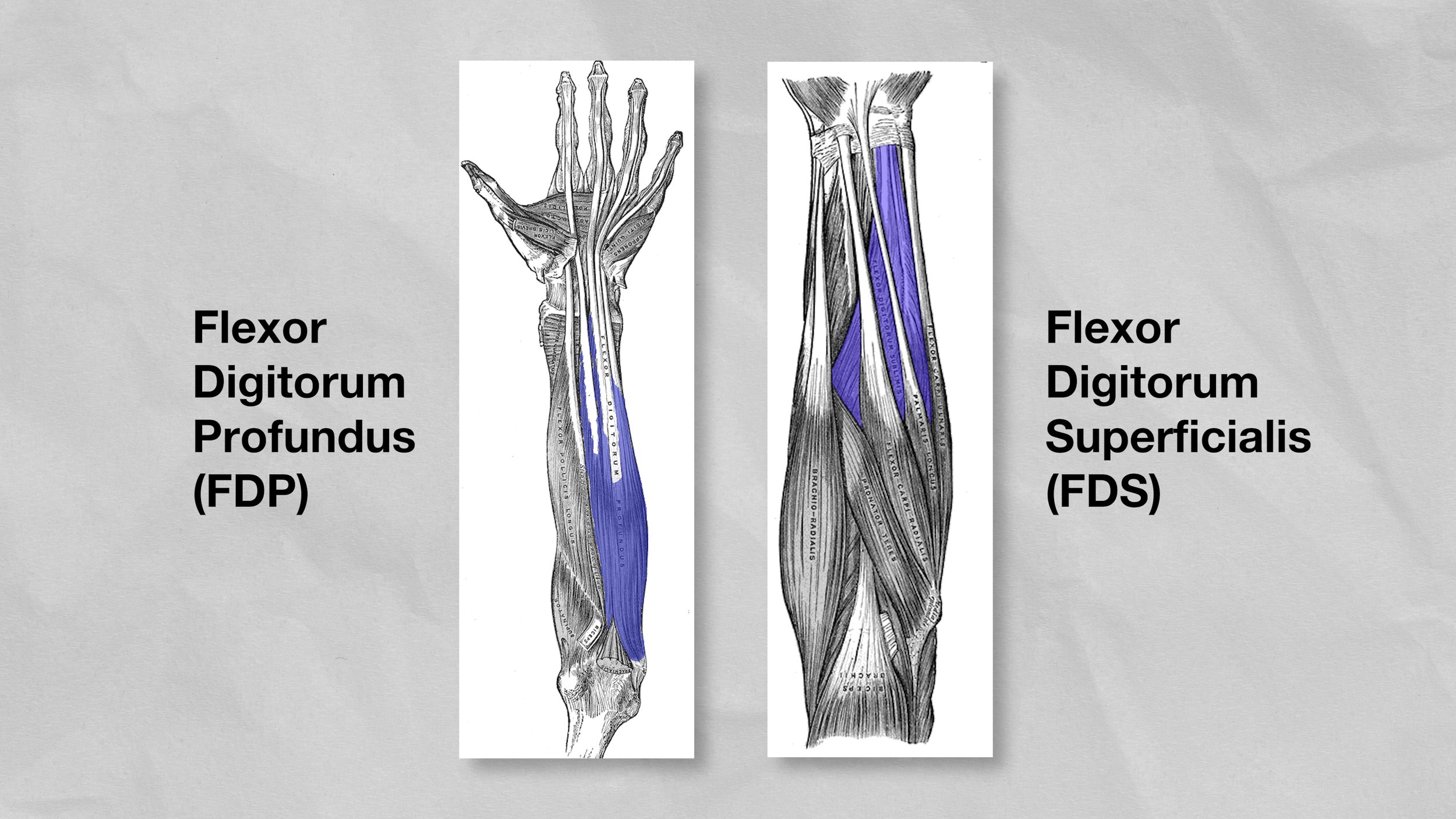
The sheaths of both the FDP and FDS can be affected by this, which we can see with the ultrasound. Looking at the FDP here, there’s a dark ring or halo around it. That halo happens because of fluid surrounding the tendon’s sheath. In an uninjured person, that halo is generally less than 2mm. If you have flexor tenosynovitis, you’ll have excess fluid in this region that makes the halo exceed 2mm. The excess fluid is actually a side effect of the irritation to the sheath; your body swells to try to protect and heal the tissue and this results in a pain response.

Now, if we were to look at a pulley injury, we might see some inflammation there as well, but if the injury is severe the obvious difference will be the increase in bowstringing, where the tendon pulls further away from the bone than it normally would because the pulley is compromised. This creates a completely different problem than what we face with flexor tenosynovitis, though it causes many similar symptoms.
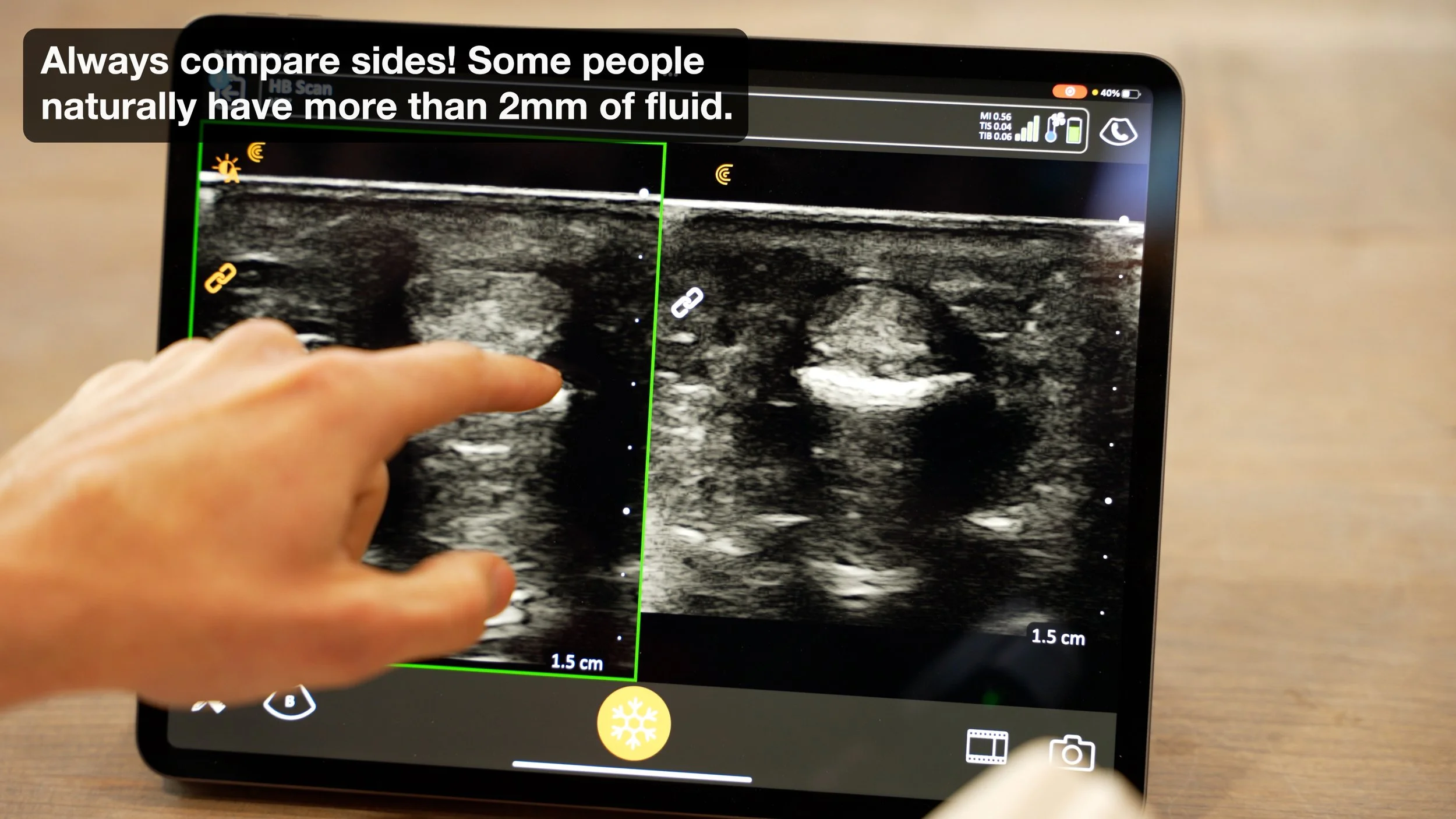
The ultrasound is extremely useful in these situations because it makes it easy to distinguish between the two injuries. It also allows you to compare between your injured and uninjured hand, which is important because some people’s halos will naturally be more than 2mm. So if you’re trying to get the most accurate diagnosis possible, I recommend scheduling an ultrasound with a clinician who understands climbing injuries. If you live anywhere near us in San Diego, you can even schedule an appointment with me! Obviously, that’s not going to be possible for everyone, though, so let’s keep going.
DIFFERENTIAL DIAGNOSIS
Differentiating from a Pulley Injury
To determine whether you have flexor tenosynovitis or a pulley injury, there are a few things you can look for that don’t require an ultrasound.
Passive Extension: Tenosynovitis will sometimes cause pain when you passively extend your finger, whereas a pulley injury will not likely not cause this.
Grip Pain: Tenosynovitis may cause pain when pulling in the open hand position, whereas this is less likely with pulley injuries.
Overuse: Tenosynovitis does not usually happen suddenly as a traumatic injury -- it tends to build up from overuse -- whereas pulley injuries can either be traumatic or overuse-related.
Forearm Pain: Tenosynovitis can sometimes cause pain in the forearm, where a pulley injury will not.




That should allow you to get a pretty good idea of which type of injury you have, but if you want to be super thorough, you should also try to rule out an injury to the tendon itself (called flexor tendinopathy). Use this chart to cross-reference all your symptoms and narrow down your diagnosis. You can screenshot it now if you’d like, but it will also be on our website (link in description as always).
Differentiating from an FDP/FDS Injury
Pain Location: Tenosynovitis will usually cause pain near the A2 and A4 pulley regions, whereas tendinopathy may be more likely to cause pain at the origin and/or insertion of the tendon.
Grip Pain: Tenosynovitis usually causes more pain in the half crimp position than it does in open hand, whereas tendinopathy of the FDP can have similar pain levels in both positions.
Palpation: Tenosynovitis can cause pain when palpating at the A2 and A4 regions, much like a pulley injury, whereas tendinopathy will not.
TREATMENT
If you think you have a pulley or flexor tendon injury, we have in-depth videos on how to treat those which we’ll link in the description.
Pulley injury: https://youtu.be/_AxN5HyBLfM
Flexor tendon injury: https://youtu.be/ub_ttbKcGvc
But if you think you have tenosynovitis, here’s what you should do.
Reduce Aggravating Factors
First, you’ll want to reduce or eliminate the aggravating factors. To do that it helps to know what created the issue in the first place.

Since we know that it’s the friction between the pulleys and tendon sheath that causes the inflammation, it’s easy to deduce the causes. The half crimp and full crimp create much more of this friction than open handed positions, so frequent crimping is the obvious culprit. Intense campus boarding on smaller rungs can also play a role, or simply subjecting your fingers to excessive repetitive forces on the wall. Remember, tenosynovitis doesn’t happen overnight, so the cause is likely something systemic in your climbing or training habits.
Reducing whatever you determine to be the most likely culprit is the first step in treatment. This doesn’t mean you need to stop climbing completely, though, in fact some research suggests that is not an effective treatment.
Manage Your Symptoms
Second, you’ll want to manage your symptoms with one or more of the following techniques.
Compression

You can use coban tape or “fingerlings” [1] to create gentle compression and help manage swelling. It can be worn overnight and with daily activities. This isn’t a miracle fix nor is it strictly necessary, but there is some scientific literature to support it as a treatment for this injury.
Tape

You can use climbing tape like a cast to immobilize your finger if you find that it helps you avoid crimping while climbing. Beyond that usage of tape, however, it’s currently unclear whether supportive taping methods like H-taping will help with tenosynovitis or exacerbate it. This is where the rehab differs quite a bit from pulley injuries, where supportive taping is generally recommended. With tenosynovitis, supportive taping could help by reducing friction from bowstringing, or it could make things worse by adding too much external compression and actually increasing friction. I’m waiting to see more evidence before I can make a strong recommendation here.
Tissue Loading
Third, you’ll want to perform safe loading of the tissue. This generally triggers tissue healing while improving blood flow and circulation.

If your injury is severe, avoid loading the tissue until the pain and swelling subsides to a more moderate level, usually within a week or so. Once you can handle day-to-day activities with minimal pain, start loading the tissue lightly with low-intensity holds (6-10 sets of 30 seconds on, 30 off), progress to open-handed farmer hangs (4-6 sets with heavier loads, 10-15 seconds on with 60-90 seconds rest) and even some low-intensity climbing if it’s well tolerated. You essentially want to load as much weight as possible without creating more than a 2/10 on the pain scale. The pain also shouldn’t linger more than a few seconds after you complete a set.

As things heal and strengthen you can slowly progress the weight and intensity, usually over a period of several weeks, eventually adding in some crimping if the pain is minimal. Just remember that tenosynovitis happens from repetitive friction, so progressing the load too quickly might not be obvious at first. Take things slow and use the rest of your training time for things that don’t tax the fingers too heavily. Many tenosynovitis injuries can be completely resolved in about 6-8 weeks, though some will take longer depending on severity and how diligent you are about rehab.

Injections
Fourth, if conservative treatment fails for more than six weeks, corticosteroid injections may be warranted. While there is inherently some amount of risk with this and thus should not probably not be the first line of treatment, the risk appears to be quite low. Results after two injections are often quite good. Corticosteroids will be the most common, but hyaluronic acid, platelet rich plasma (PRP), and NSAIDS are also possibilities.[3]

Other Forms of Treatment
Finally, there are several other treatments you can try for managing your symptoms and promoting healing, though I don’t find any of them to be particularly compelling at this time. I’m listing them here so you can try them out for yourself if you like, though, as they present little to no risk and could have a positive effect.
Blood Flow Restriction: In theory this sounds useful, as you’d be able to stimulate the tissue as if it’s under higher load without actually using high loads, but the research on BFR for climber-related issues is quite limited and it requires extra equipment and know-how to perform.
Ice Therapy: Personally I’ve never been a huge fan of icing, but if you are experiencing visual swelling then it may be beneficial.
Finger Splints: I’m never a huge fan of splinting / immobilization unless it is just to avoid crimping.
Local Ointments: Similar to icing, never been a huge fan of this. I’d rather treat the cause (over crimping, over training) than just put an ointment on it. But if it helps with the inflammation then go for it.
Acupressure Rings: The use of acupressure rings or other devices to lightly stimulate the area has been proposed to improve blood flow and help with healing
Putty: Gentle gripping such as with putty to improve blood flow has also been proposed.
Leeches?! In the Schoeffl paper, they note that leech therapy for treatment-resistant patients proved to be a valuable alternative with no complications [3]. Interesting!
CONCLUSION
As the research grows we may be able to recommend more specific guidelines, but for now the most important aspect to understand with your training is prevention. Monitor your volume and intensity, frequency of climbing, grip styles, etc. A balanced approach may prevent you from ever having to worry about this issue. But, if you are suffering from it, hopefully this video and recommendations have helped.
If you have experienced this, be sure to share your story in the comments below!
Train. Climb. Send. Avoid flexor tenosynovitis. Repeat!
DISCLAIMER
As always, exercises are to be performed assuming your own risk and should not be done if you feel you are at risk for injury. See a medical professional if you have concerns before starting new exercises.
Written and Presented by Jason Hooper, PT, DPT, OCS, SCS, CAFS
IG: @hoopersbetaofficial
Filming and Editing by Emile Modesitt
www.emilemodesitt.com
IG: @emile166
CITATIONS
Mohn S, Spörri J, Mauler F, Kabelitz M, Schweizer A. Nonoperative Treatment of Finger Flexor Tenosynovitis in Sport Climbers-A Retrospective Descriptive Study Based on a Clinical 10-Year Database. Biology (Basel). 2022;11(6):815. Published 2022 May 25. doi:10.3390/biology11060815 [1]
Lutter C, Tischer T, Schöffl VR. Olympic competition climbing: the beginning of a new era-a narrative review. Br J Sports Med. 2021;55(15):857-864. doi:10.1136/bjsports-2020-102035 [2]
Schöffl V, Strohm P, Lutter C. Efficacy of corticosteroid injection in rock climber's tenosynovitis. Hand Surg Rehabil. 2019;38(5):317-322. doi:10.1016/j.hansur.2019.07.004 [3]