Ultimate A2 Pulley Injury Recovery Guide (PT's Full Protocol)
Hooper’s Beta Ep. 167
Introduction
The A2 pulley is not only the most commonly injured pulley in climbers, it’s the most common type of finger injury in climbers. Years ago we created an in-depth guide for A2 pulley injury recovery, but now it’s time for an update! This guide contains a multitude of improvements, including:
Changes to the recovery exercises
New differential assessment tools
A fun demonstration to illustrate why crimping causes A2 injuries
More scientific research references and citations
And a brand new guide on how to integrate climbing throughout your recovery
You’ll learn everything you need to know about A2 injuries from identifying the symptoms all the way to getting back on the wall pain-free. And don’t forget, if you don’t like the idea of DIYing your recovery, you can always use our super affordable Recovery Blueprints, which are pre-built recovery programs made specifically for climbers.
As always, if you appreciate the effort we put into making free quality content for climbers, consider purchasing from our affiliate links or our very own webstore.

🔗 Useful Links
👉 Recovery timelines and climbing guidelines for grades I-IVa: https://drive.google.com/drive/folders/1462Uwlni2H7YrHpkQLHDXpGAecOhJHqw?usp=sharing
👉 Our new adjustable pulley splints: https://www.hoopersbeta.com/store/p/pulley-splint
👉 Free STL files for pulley splints: https://www.hoopersbeta.com/store/p/pulley-splint-files
👉 Our training / recovery products: https://www.hoopersbeta.com/store/our-products
👉 Schedule a consult with Dr. Jason Hooper, PT, DPT, OCS, SCS: https://www.hoopersbeta.com/private-sessions
What Causes an A2 Injury?
The A2 pulley is a short band of connective tissue in the proximal segment of our fingers that helps keep the flexor tendon in place under load. During intense gripping, the A2 encounters immense load as the flexor tendons press up against it. Under the right (or rather, wrong) circumstances, the A2 can be injured in one of two ways:
A sudden tear from too much force all at once, which we call an “acute” injury
A slower build-up of inflammation due to highly repetitive activity, which we call a “chronic overuse” injury.
Acute

For acute injuries, the tear can be anywhere from very small (grade I) to full rupture (grade III) or, in extreme cases, full rupture of multiple pulleys in one finger. This can happen to a perfectly healthy pulley, like if your foot unexpectedly slips off a hold resulting in a sudden overload of a finger. Unsurprisingly, though, the likelihood of an acute injury tends to increase if the pulley is already slightly compromised, such as from an underlying overuse issue.
Chronic

For chronic overuse injuries, the accumulation of minor tissue damage from intense, repetitive gripping leads to persistent inflammation, reduced tissue integrity, and pain. Examples of this are frequently seen in climbers who suddenly start board climbing multiple times per week or who add too much hangboarding all at once without reducing load in other areas. Chronic overuse injuries with pulleys are quite common, though if you’ve been struggling with yours for more than roughly 8-10 weeks, you should actually look into a different category of injury called “pulley thickening.” We have a full length video on this topic, which we prefer to call “injury-induced pulley thickening” for reasons explained in the video.
An Interesting Hypothesis About Pulley Injury Risk (and a Warning)
There are multiple factors that can determine someone’s chances of getting a pulley injury, like grip preferences, training history, training habits, and genetics. These things can make you more or less prone to this type of injury by affecting how strong your pulleys are, how healthy they are, and how much force they encounter on the wall. However, there may be more direct or immediate mechanisms of pulley injuries as well.
One hypothesis is that if your grip opens up under heavy load, the pulley encounters a huge amount of friction as the flexor tendon slides past it. That friction could be what causes micro-trauma to pulley, reducing its ability to handle load with chronic repetition. The friction is partially caused by directional ridges on the pulleys, kind of like how cats have those spines on their tongues that make them rough in one direction but smooth in another. This helps us “lock in” to a crimp under heavy load without making it hard for the two structures to slide past each other when you’re just moving your fingers.
What’s even more intriguing, though, is that some people may have more friction than others. It could actually be an advantage for grip strength, but it could also make pulley injuries more likely (kind of like scraping extra hard against an extra spiny cat tongue).
The exact amount this phenomenon actually contributes to pulley injuries is still unclear, but I think it’s worth paying attention to how frequently you allow your hand to open up on hard crimps. I generally advise climbers to avoid this as there does seem to be a correlation with pulley injuries. Exercises like crimp curls seem to be okay (or even beneficial) because the load is so much lower, but opening up under very high loads is not advisable.
Why Does Crimping Cause A2 Pulley Injuries?
The forces acting on the pulleys significantly change depending on the angle of our finger joints while gripping. This was demonstrated by Vigouroux et al² when they compared a crimp grip to a more open-handed drag or chisel-like grip (which they strangely refer to as a “slope grip”).
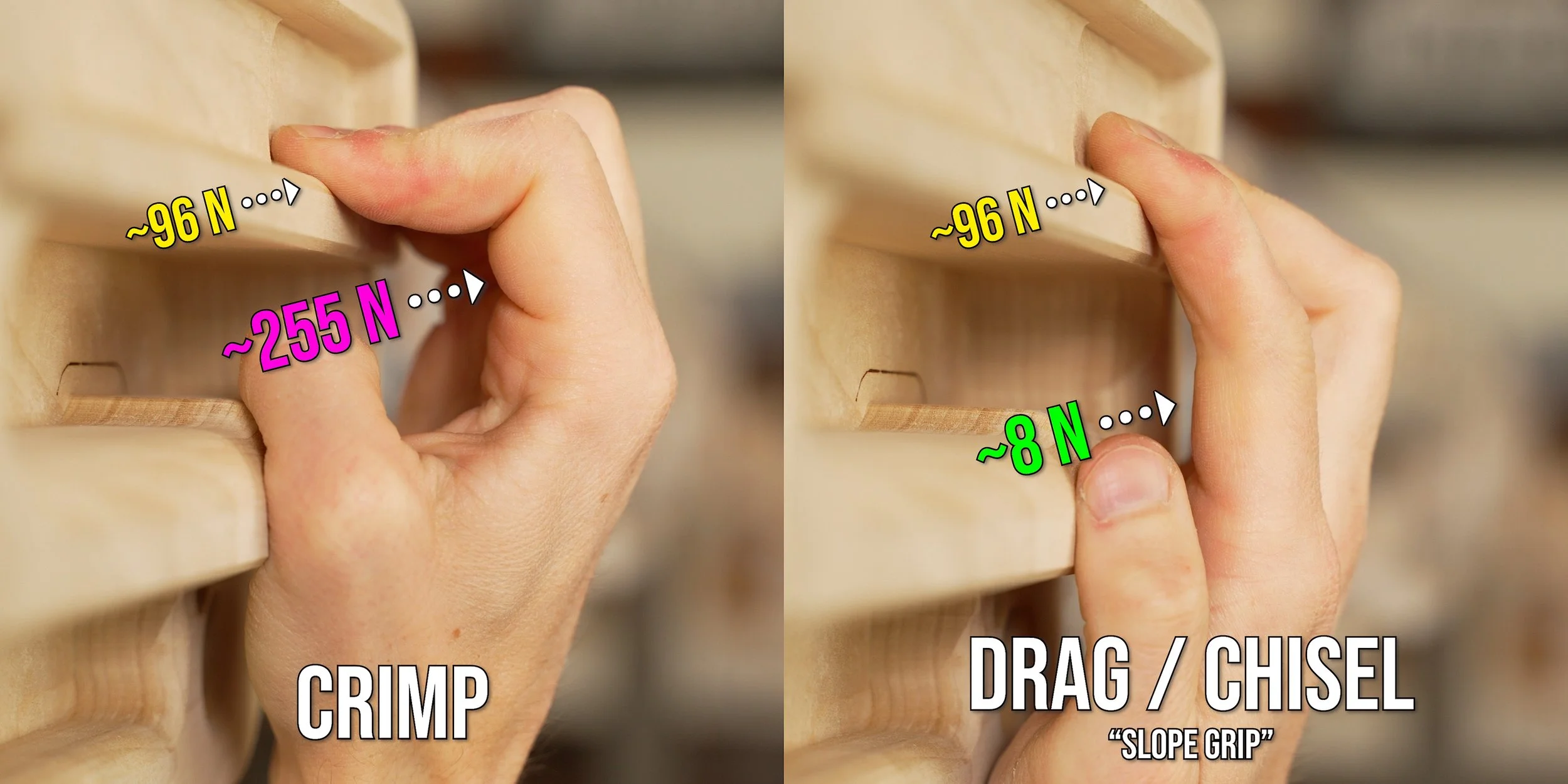
In the crimp position, when about 96 Newtons of force was applied to the fingertip, the A2 pulley experienced about 255 Newtons of force. But in the more open-handed position, the A2 pulley only experienced about 8 Newtons of force. That’s about a 97% reduction in force on the A2 pulley by going from a crimp position to a more open-handed one! How is that possible?
It all has to do with the biomechanical changes that occur when we bend our fingers.
The amount of force the A2 pulley encounters is vastly different depending on the grip position, even when the force on the flexor tendons remains the same.
Note: Important demonstrations are show in the video, please watch the full video for a deeper understanding.
So Crimping is Canceled!?
Before you start calling all your friends to tell them crimping is dangerous and they should basically never do it, I want to make one thing clear: you can (and should) increase the strength of your pulleys with proper training so they become more than capable of handling these high forces. There is way too much fear mongering out there about crimping, so let’s not add to it with blanket statements like “crimping is dangerous.” That’s like telling someone they shouldn’t sprint because a hamstring strain is more likely compared to walking. Sprinting obviously isn’t bad, it's just a high intensity exercise that requires training.
What Does an A2 Injury Feel Like? (Symptoms and Severity)
Let’s identify the signs and symptoms so you can determine the severity of your injury, which will determine what your recovery looks like.
Remember in the beginning when I mentioned that free tool? We spent countless hours creating a finger injury assessment on our website to help you understand the type *and* severity of your injury. Simply answer a series of multiple choice questions and get a result! Please note this is for educational purposes only and is not a substitute for professional medical advice or diagnosis, but it’s an awesome way to jumpstart your injury knowledge. Did I mention it’s free? Link in the description or go to hoopersbeta.com/finger-tool.
A2 Pulley Injury Severity Guide
Chronic Overuse
A chronic overuse injury typically presents as discomfort/pain in the middle of the proximal phalanx or the distal edge of your A2 pulley. Symptoms will typically occur after climbing or specifically after strenuous crimping, and may be worse the next morning but will subside after some you get moving. There will be no swelling, but palpating directly over the A2 region might feel mildly tender. Grip strength will be largely unaffected in more open-handed positions and you might only notice a small reduction in strength on more aggressive crimps. This might improve as you warm-up, but then cause you more pain later. The lack of significant strength loss or immediate pain often leads to people ignoring this issue until it gets worse.
Grade I (Acute Mild Sprain)

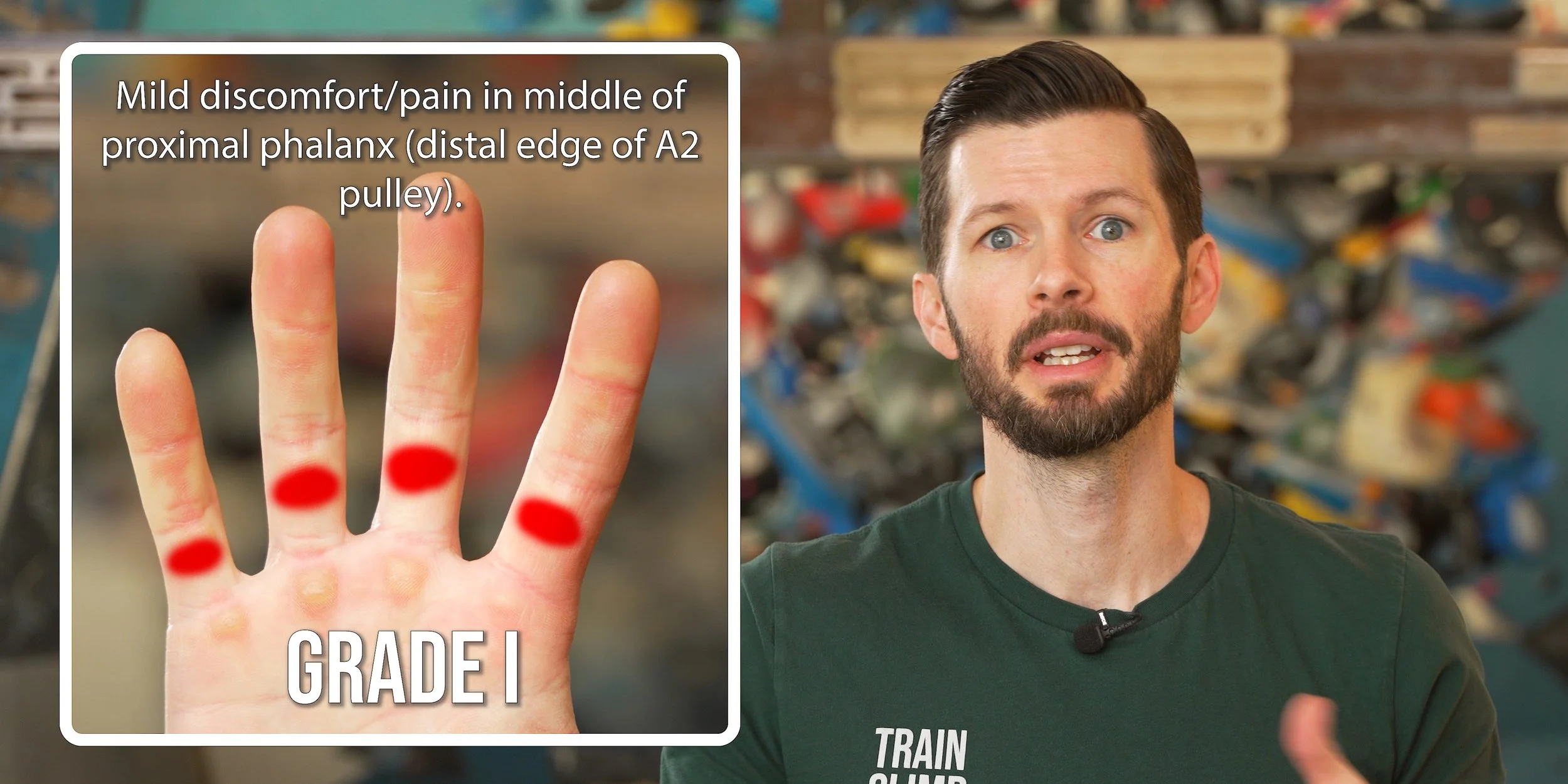
A grade I A2 injury, also known as an acute mild sprain, typically presents as discomfort/pain in the middle of the proximal phalanx or the distal edge of your A2 pulley. This is technically a small tear of the pulley, but we call it a “sprain” to help differentiate it from more severe injuries. Grade I symptoms usually appear suddenly following intense or repetitive crimping. The pain tends to subside by the next day, but will resurface as soon as you start crimping again. There will be no swelling, but palpating directly over the A2 region might feel mildly tender. Grip strength will be largely unaffected in more open-handed positions but will be reduced when crimping. The lack of significant strength loss, especially in open-handed positions, can deceive some people into thinking it must be okay to climb hard and ignore the pain, which unfortunately may worsen the injury or cause other subsequent issues.
Grade II (Acute Partial Tear)

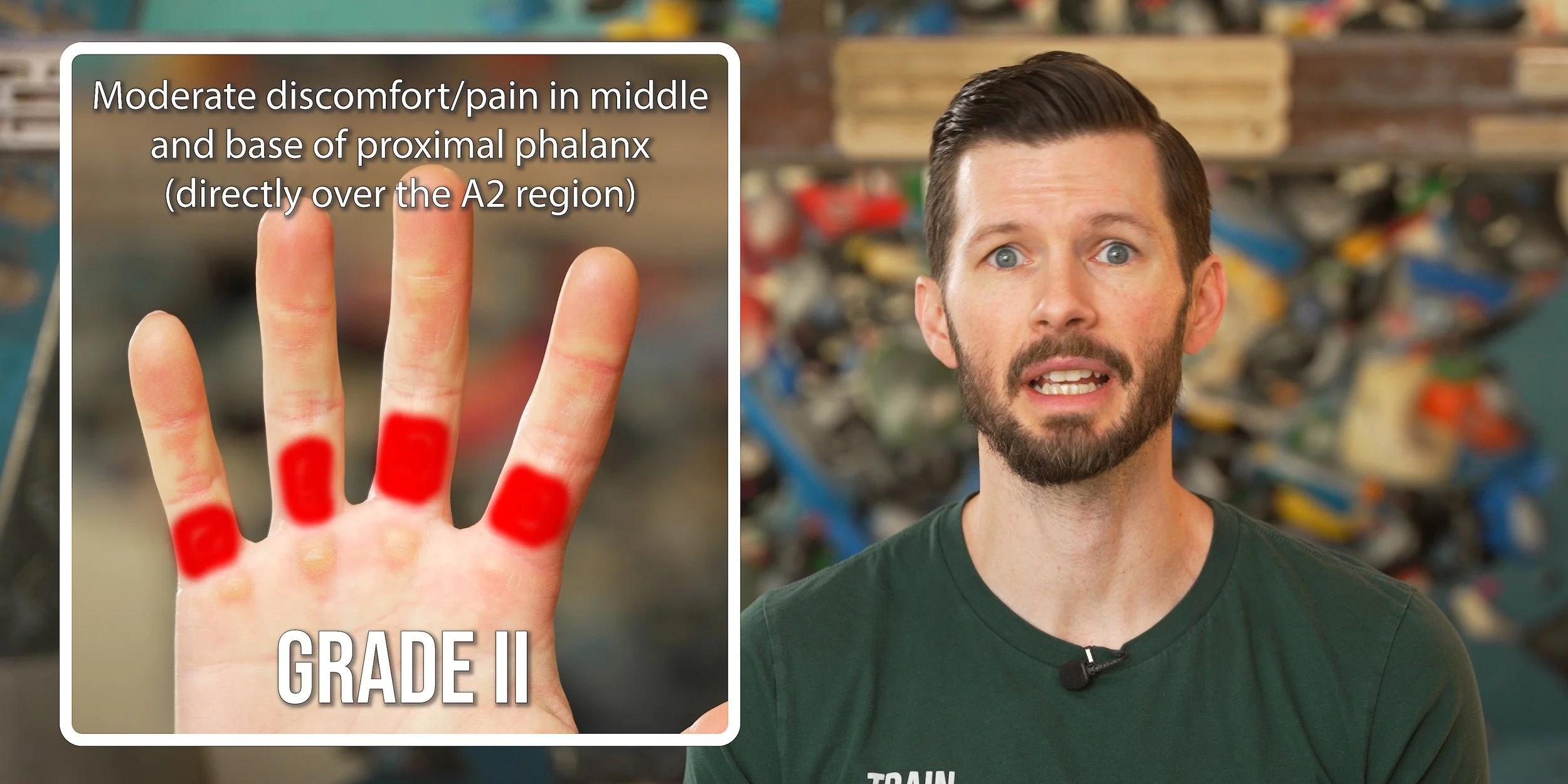
With a grade II A2 injury, or acute partial tear, the pain is more pronounced and tends to linger for multiple days after initial onset or aggravation. Pain from palpation will be sharper and a small amount of swelling in the A2 region can sometimes develop. The swelling will not always be visually obvious; sometimes it is felt more than seen. It’s not uncommon for the finger to feel an increase in stiffness when you wake up in the morning, and it may feel noticeably weaker or more sensitive even on larger holds. All grip positions will exacerbate the pain when loaded. A flap tear is possible with a grade II injury, so be sure to read that section after we explain the rest of the grades.
Grade III (Acute Rupture)

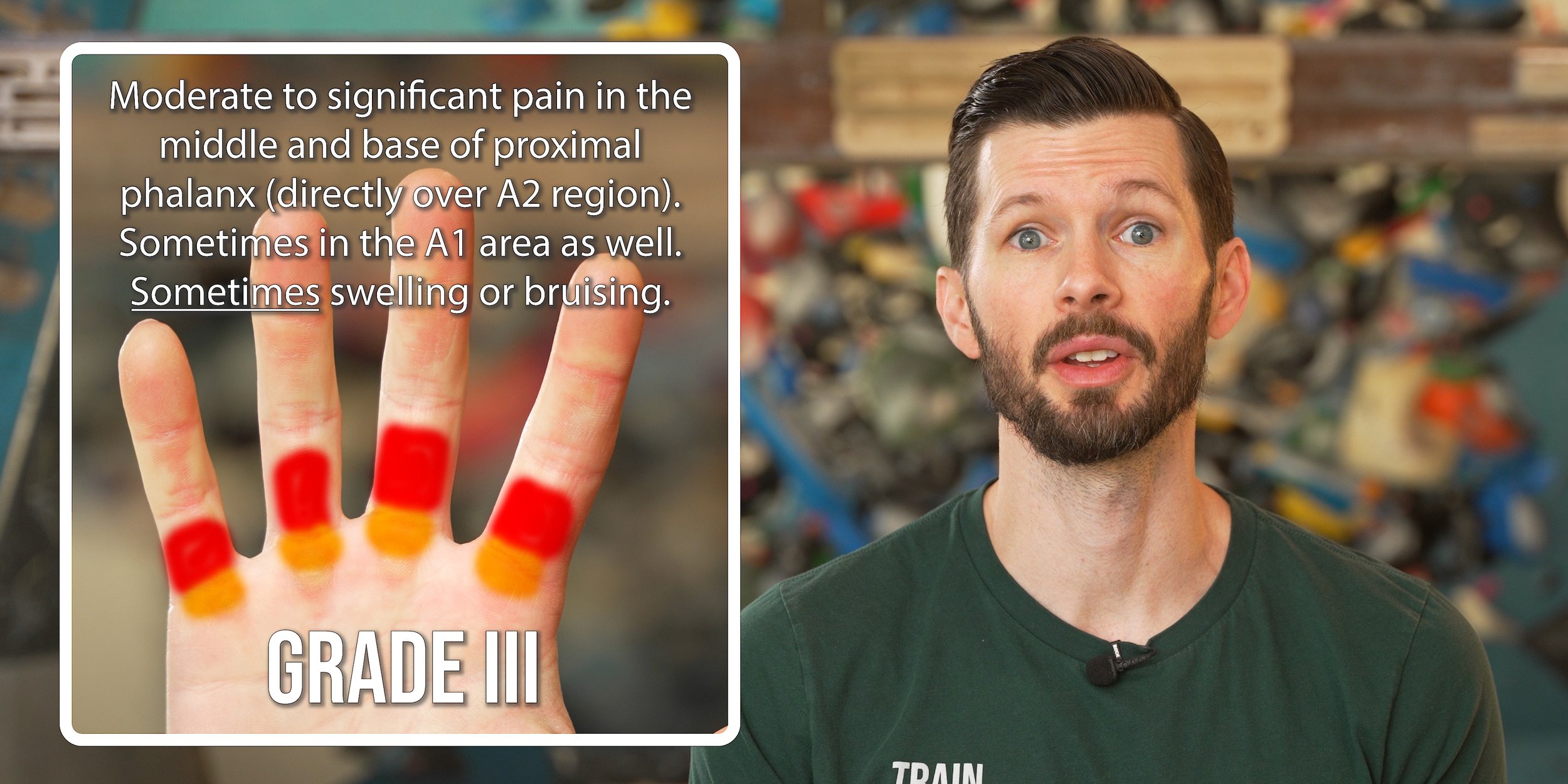
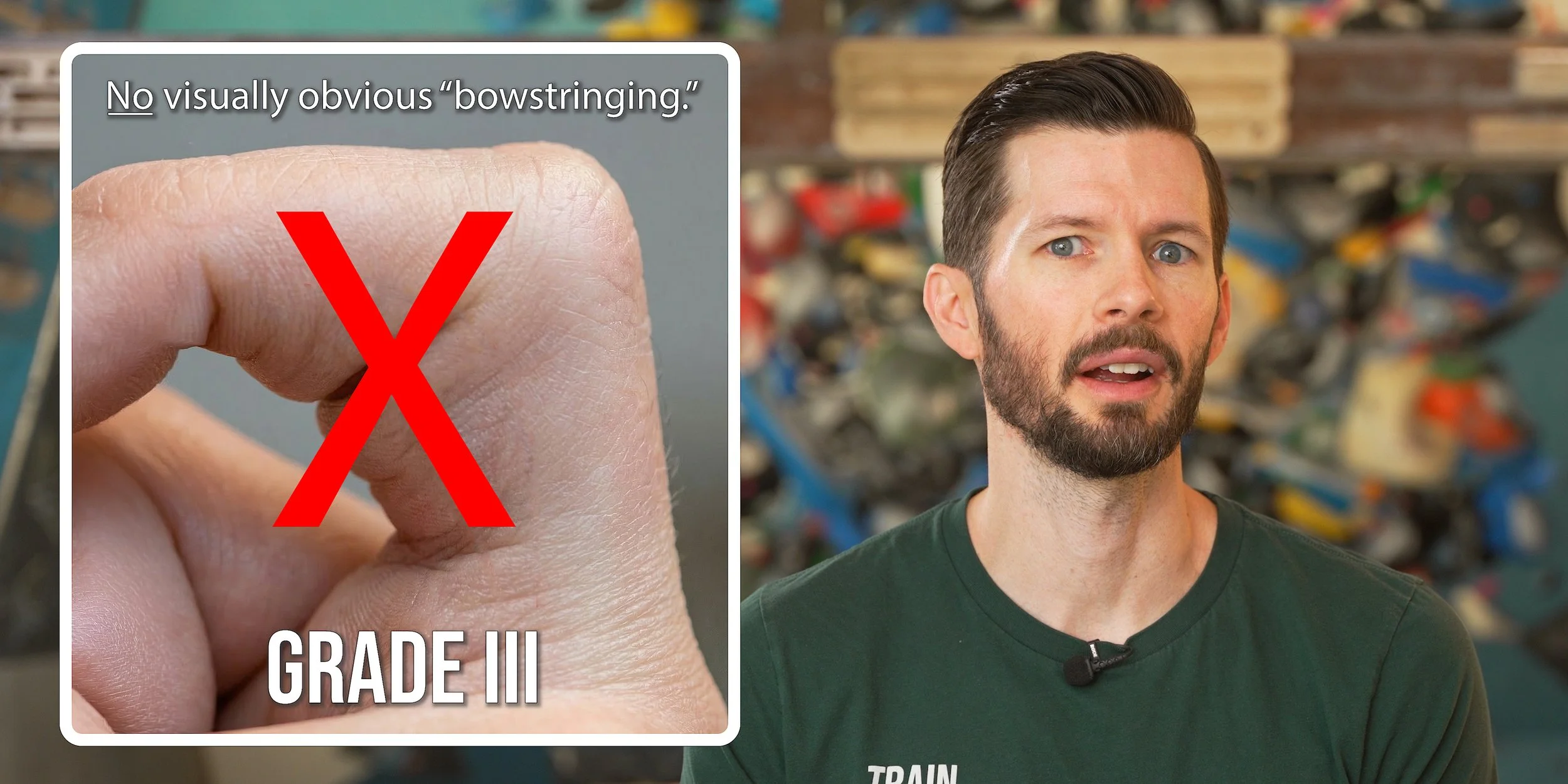

A grade III A2 injury, or complete rupture, typically involves a distinct popping sound or tearing sensation at the moment of injury. Pain or discomfort can immediately follow, though it may not start until the inflammation sets in, which may take hours. Swelling and bruising can appear within minutes to a few hours, though it will not always be present. This is important: you can still have a grade III injury even if you have no visually obvious swelling or bruising. Similar to a grade II injury, swelling may be felt more than it is seen, but it still may not be obvious. Grip strength will be significantly reduced, likely in all grip types and sometimes day to day activities. But, sometimes the pain is not what you would expect; you may not have any pain even on crimps, except with very high forces. This again may be misleading as you might think nothing is wrong, but the lack of pain is simply because there is no remaining pulley to cause a pain response. Most people will experience a reduced range of motion, though, which is typically worse in the morning. Despite the full tear, there will still be no bowstringing that you can see with your naked eye. However, bowstringing will be visible with MRI or ultrasound. A flap tear is possible with a grade III injury.
Grade IV (Acute Rupture of Multiple Pulleys)

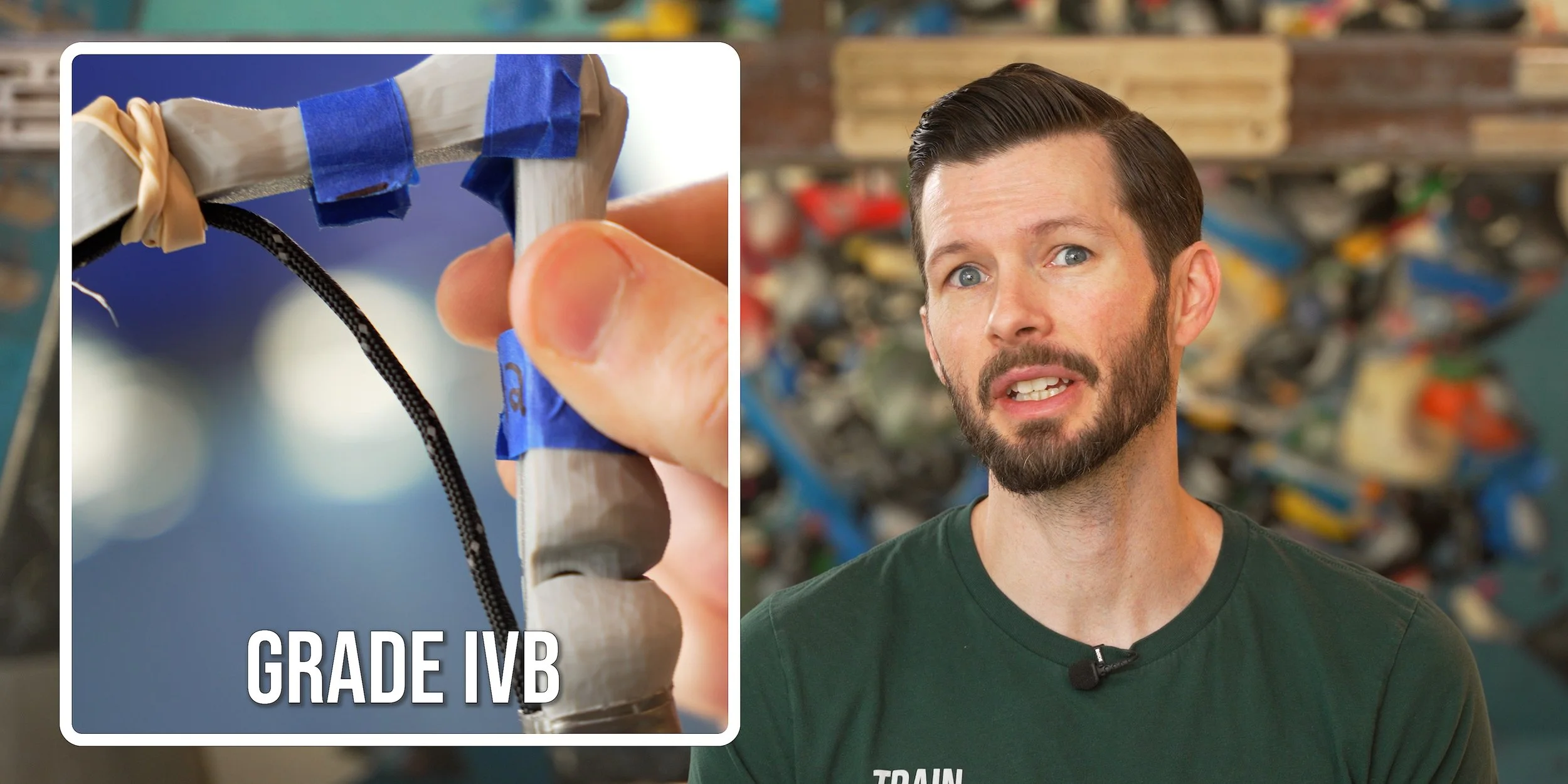
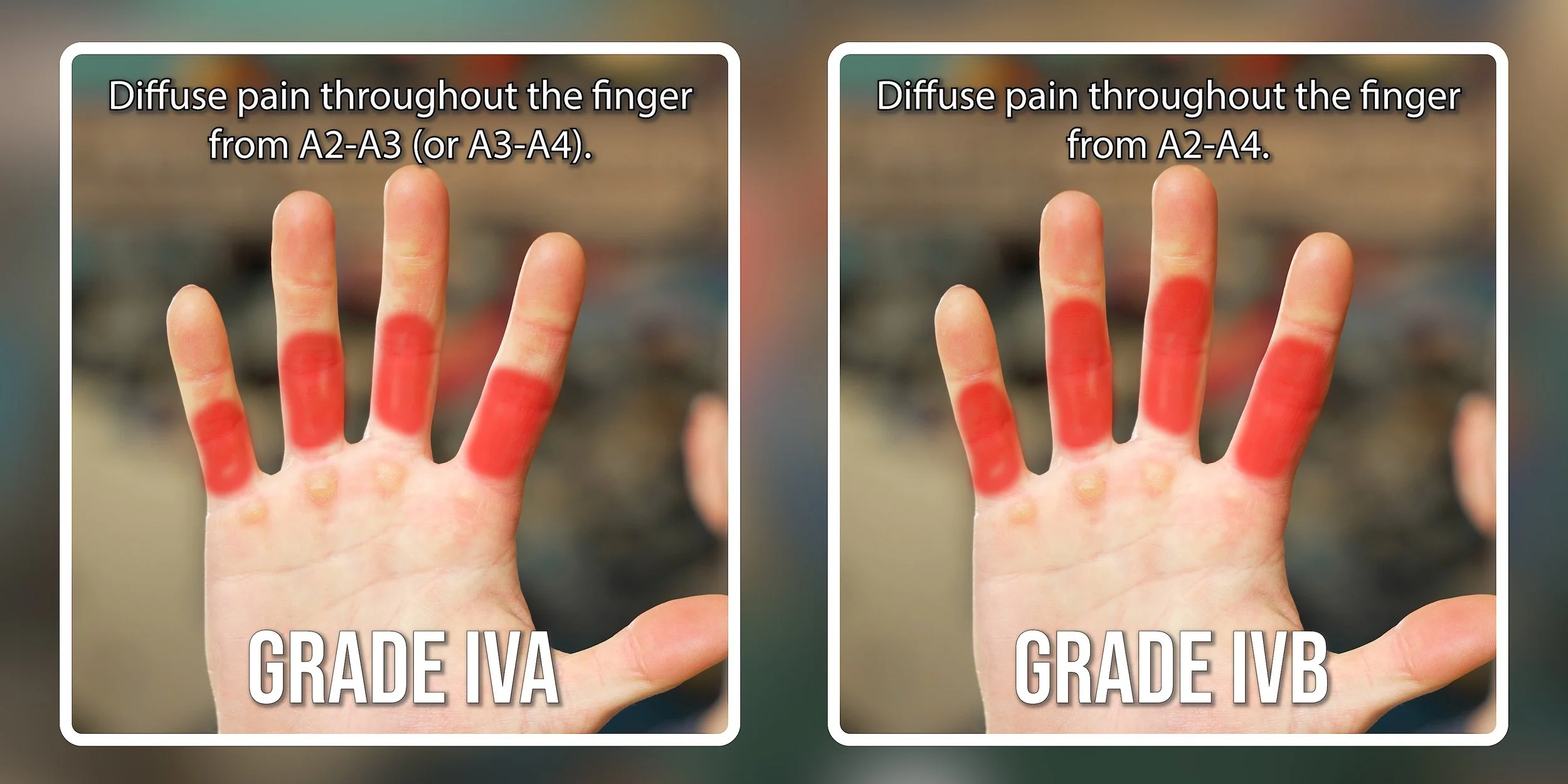
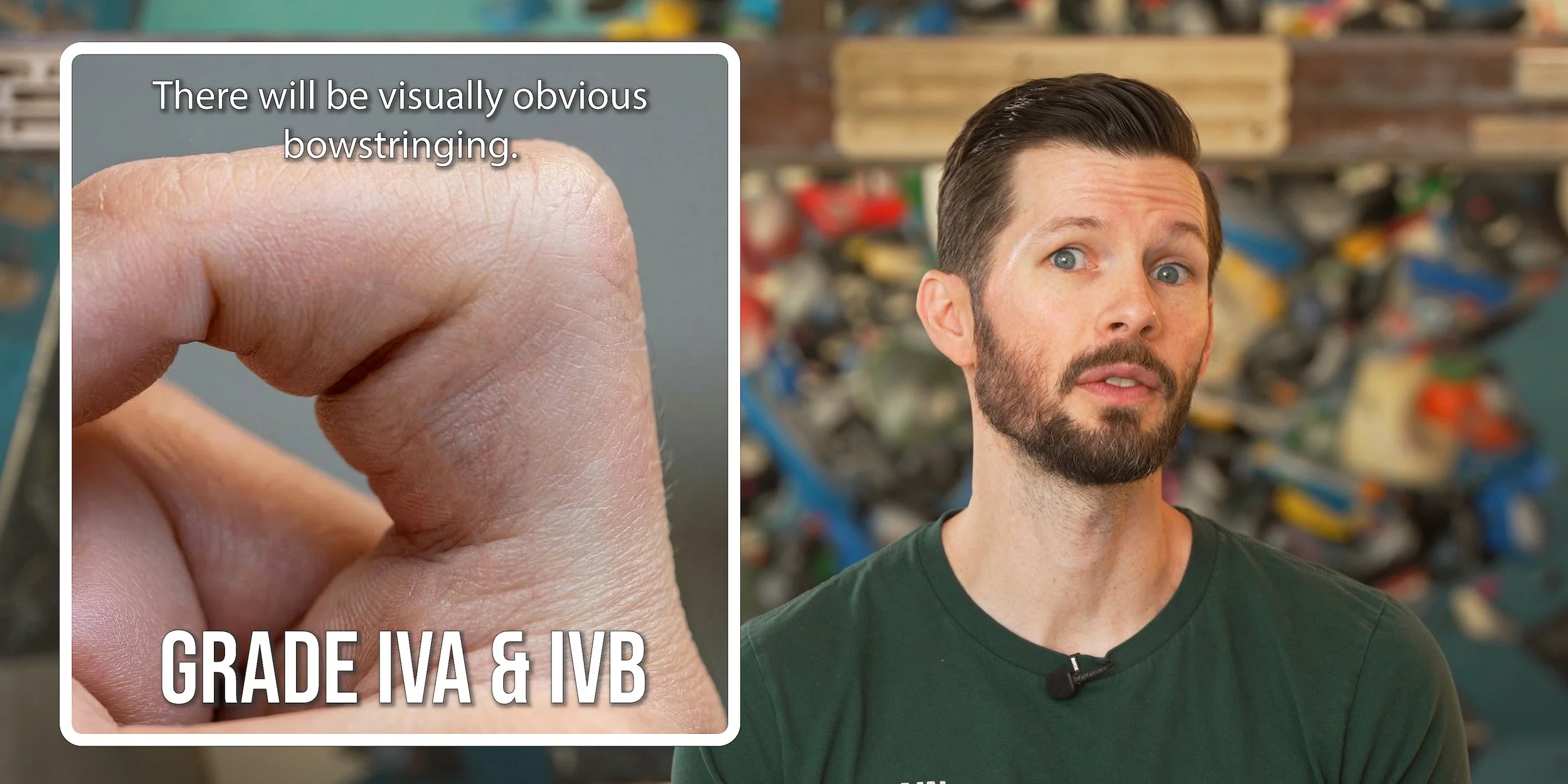
A grade IVa injury is a complete rupture of the A2 and A3 pulleys (or A3 and A4), while a grade IVb tear is a complete rupture of A2, A3, and A4. A grade IVb tear requires surgical consultation and thus will not be covered in this blog. If you suspect a grade IVb injury, you should reach out to a skilled professional. All grade IV tears involve one or more distinct popping sounds or tearing sensations at the moment of injury. Pain or discomfort is likely to follow immediately, and may worsen as swelling and inflammation sets in, which may occur within minutes or hours. Swelling and bruising are likely. Grip strength will be significantly reduced with all grip types and activities of daily living. A reduction in range of motion is also to be expected. Bowstringing will be visible to the naked eye (as well as with MRI or ultrasound). Flap tears are also possible with grade IV.
What is a Flap Tear?
A flap tear occurs when the torn pulley gets wedged underneath the flexor tendon sheath after a Grade II, III, or IV injury. The flap rubs against the tendon sheath as you move your finger, which causes excess friction that can lead to a separate issue called flexor tenosynovitis. We call this “flap irritation phenomenon” or FLIP for short [Schöffl].
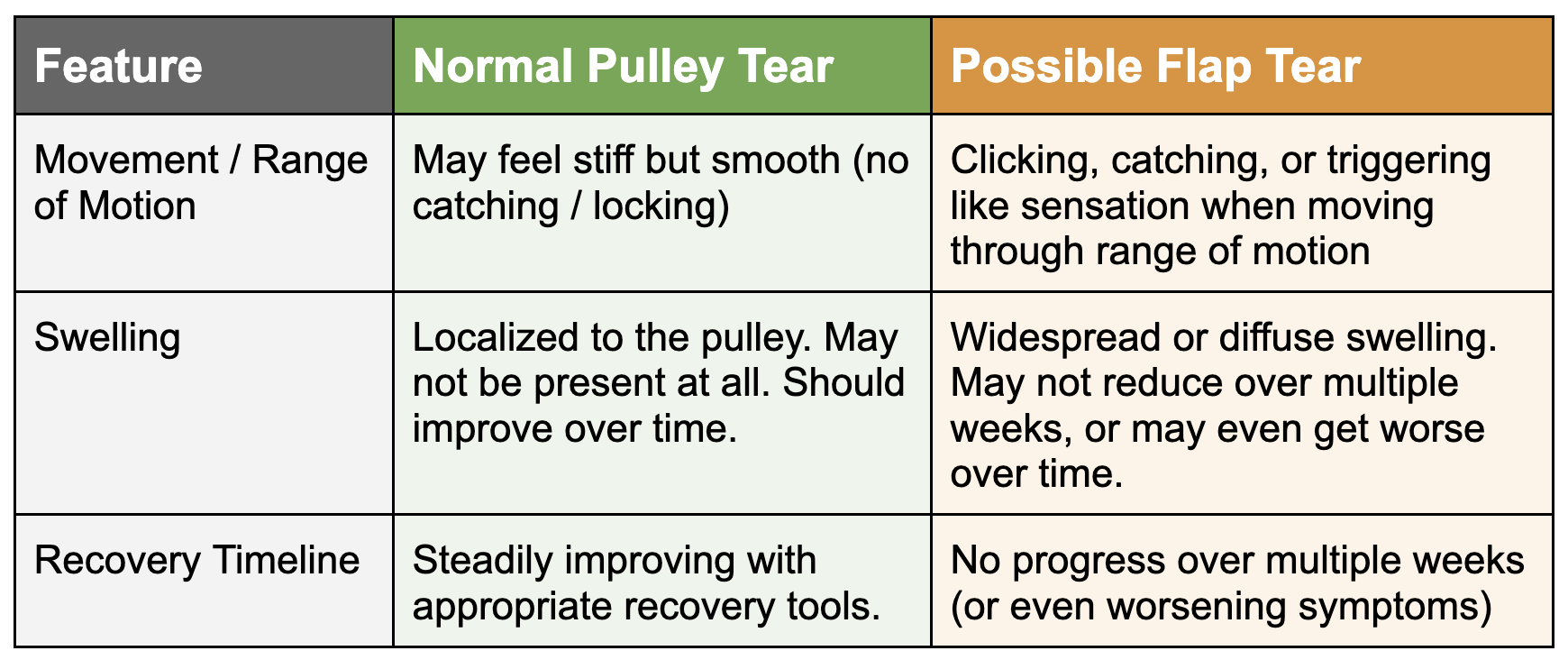
To determine if you have a flap tear, ultrasound or MRI is ideal, but here are some signs to look out for:
Mechanical catching: Physical clicking, catching, or triggering sensation in the injury area when flexing or extending the finger. Be sure to differentiate this from clicking in other areas such as your joint.
Chronic swelling: While some swelling may be normal and timelines will vary from person to person, persistent swelling that does not improve after a couple of weeks, that is present in a larger area of the finger rather than localized to the injured pulley, or that seems to be worsening over time rather than improving, is another indicator of a flap tear.
Prolonged timeline: Time itself can be a tertiary indicator. If you are not making any progress over multiple weeks, or if your symptoms appear to be worsening, and that is accompanied by increased swelling or catching, you may have a flap tear.
If you have been following a decent recovery protocol for 6 to 8 weeks since your injury and your finger is still globally swollen, catching when you bend it, or stalled in its progress, it is time to get diagnostic imaging. A flap tear may require surgery if it does not improve with conservative care.
Here is a quick reference chart to compare a normal tear with a flap tear:
How Do I Differentiate an A2 Injury from Other Injuries?
To ensure you perform the best recovery protocol possible, it’s important you make sure you’re not mistaking some other kind of finger injury for an A2 injury. If your symptoms and mechanism of injury line up exactly with what we’ve laid out so far, then you can be pretty confident you do indeed have an A2 injury. If you’re not so sure, though, you should do some further investigation. Our free finger injury self-assessment can be quite helpful for that since it has multiple questionnaires specifically for differentiation. However, as always, this does not count as medical advice or professional evaluation. For quick reference, here are the other injuries you’ll need to consider:
Injury-induced pulley thickening (IIPT), which is a gradual build-up of disorganized, inflamed tissue that leads to noticeable thickening of the pulley under the skin. Note that injury-induced pulley thickening is a term we came up with to help differentiate this type of injury from normal/benign pulley thickening. In the broader medical community, this injury is confusingly referred to as simply “pulley thickening,” which we don’t like because it makes it sound like all pulley thickening equals an injury (not true!). We have a full length video on this injury in case it applies to you.
Flexor tenosynovitis, which is chronic irritation of the sheath that surrounds the flexor tendons.
A lumbrical strain, as these can cause referred symptoms into the A1/2 region.
An FDP tendon strain, though this is less likely to cause symptoms just in the A2 region.
A “flap tear” of the pulley, as noted above.
Important: For climbers under 18 years old, pain in the finger should not be assumed to be a pulley injury. Any pain in this region must be treated as a potential epiphyseal (growth plate) fracture until cleared by a specialist. Reminder: This information is intended for adult audiences only and is explicitly not meant as medical advice for minors.
What’s the Prognosis?
As a climber myself, I know that pulley tears can be scary, but with appropriate recovery steps you’ll have nothing to worry about in the long run. I’ve treated so many of these, and when recovery is taken seriously, climbers not only return to full strength, they often come back stronger than before due to the structured training regimen.
The exact timeline can vary wildly depending on the quality of your recovery efforts, athletic background, genetics, etc.
For grade I injuries, you can expect a return to full strength in about 6-8 weeks.
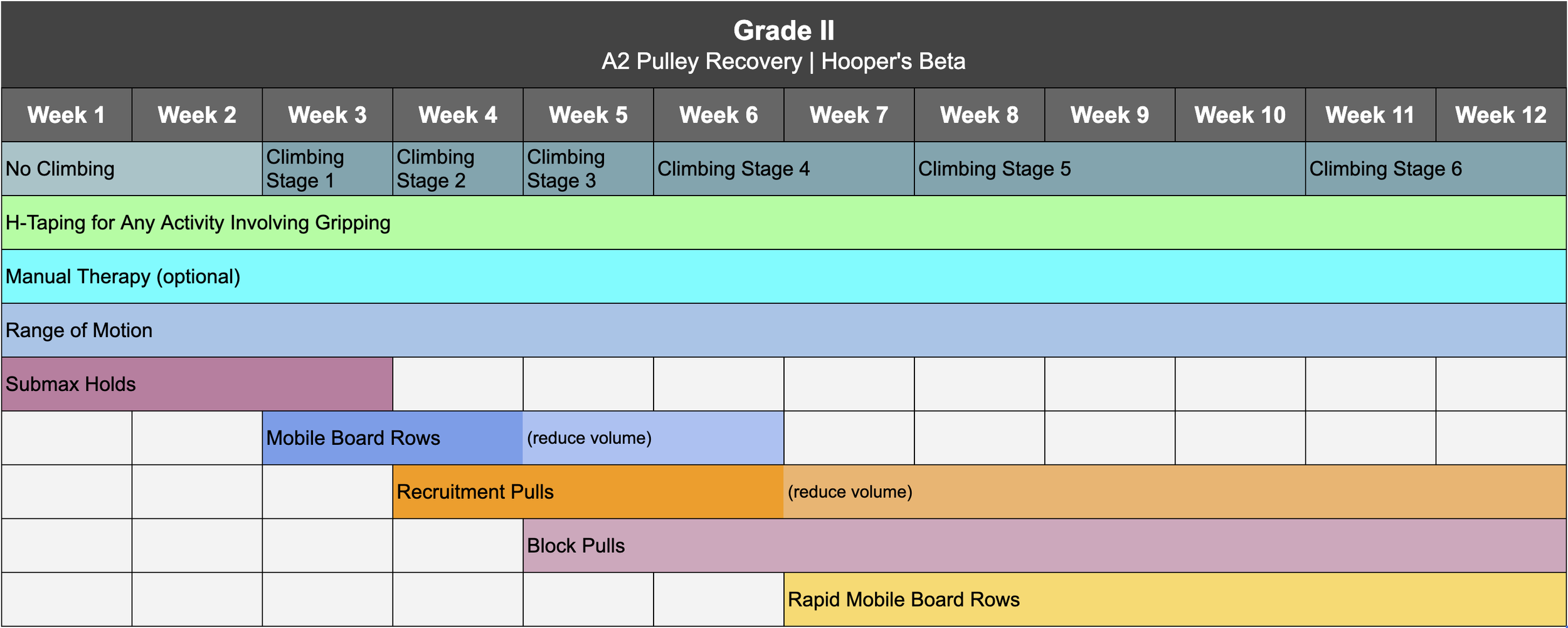
For grade II injuries, think more like 10-12 weeks.
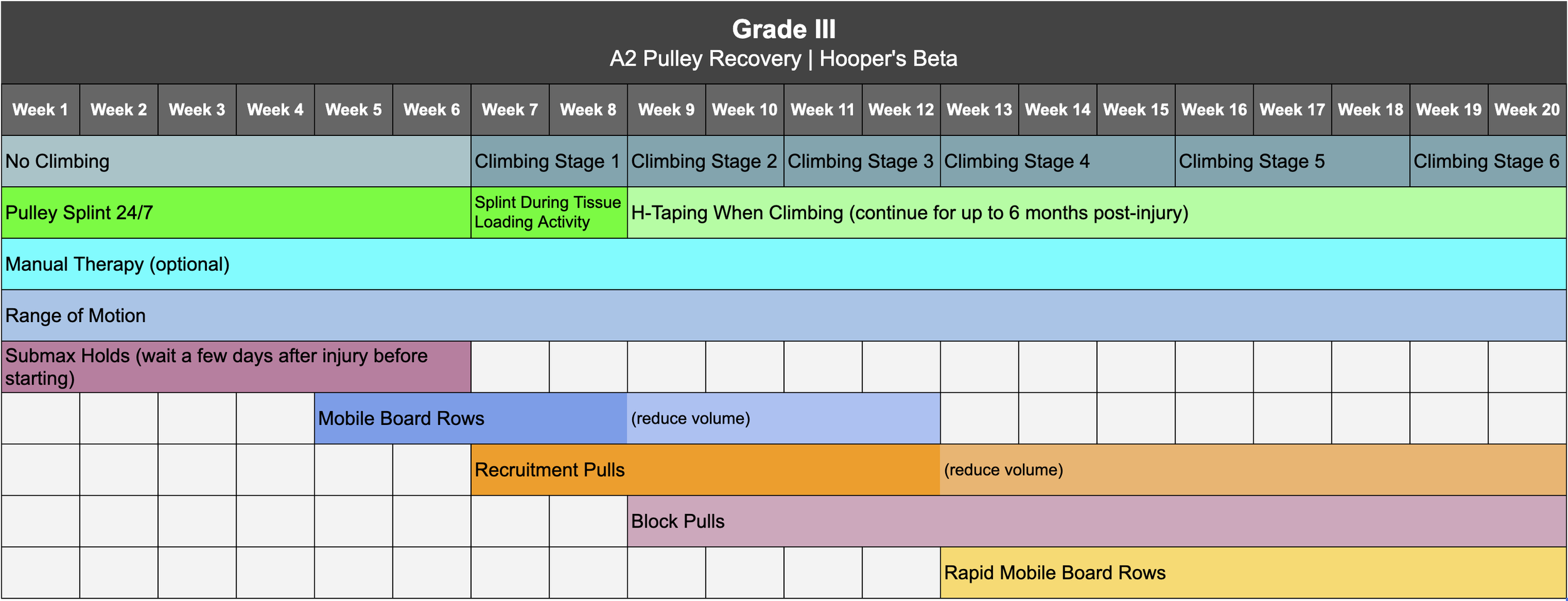
For grade III, it will be a bit more gradual – as little as 16 weeks for some, but typically about 20 weeks or a bit longer for a full comeback.
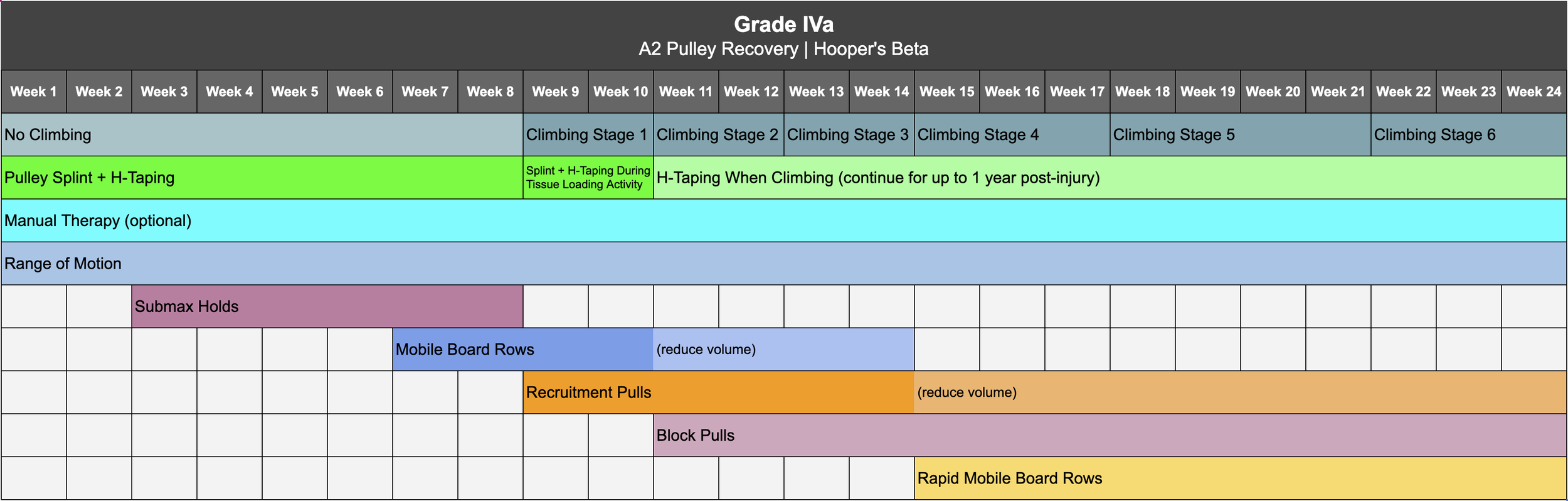
Grade IVa injuries can take as little as 24 weeks for some individuals, but may take up to an entire year for a full recovery.
For grade IVb, this will depend on your surgical team and protocol.
How Do I Recover?
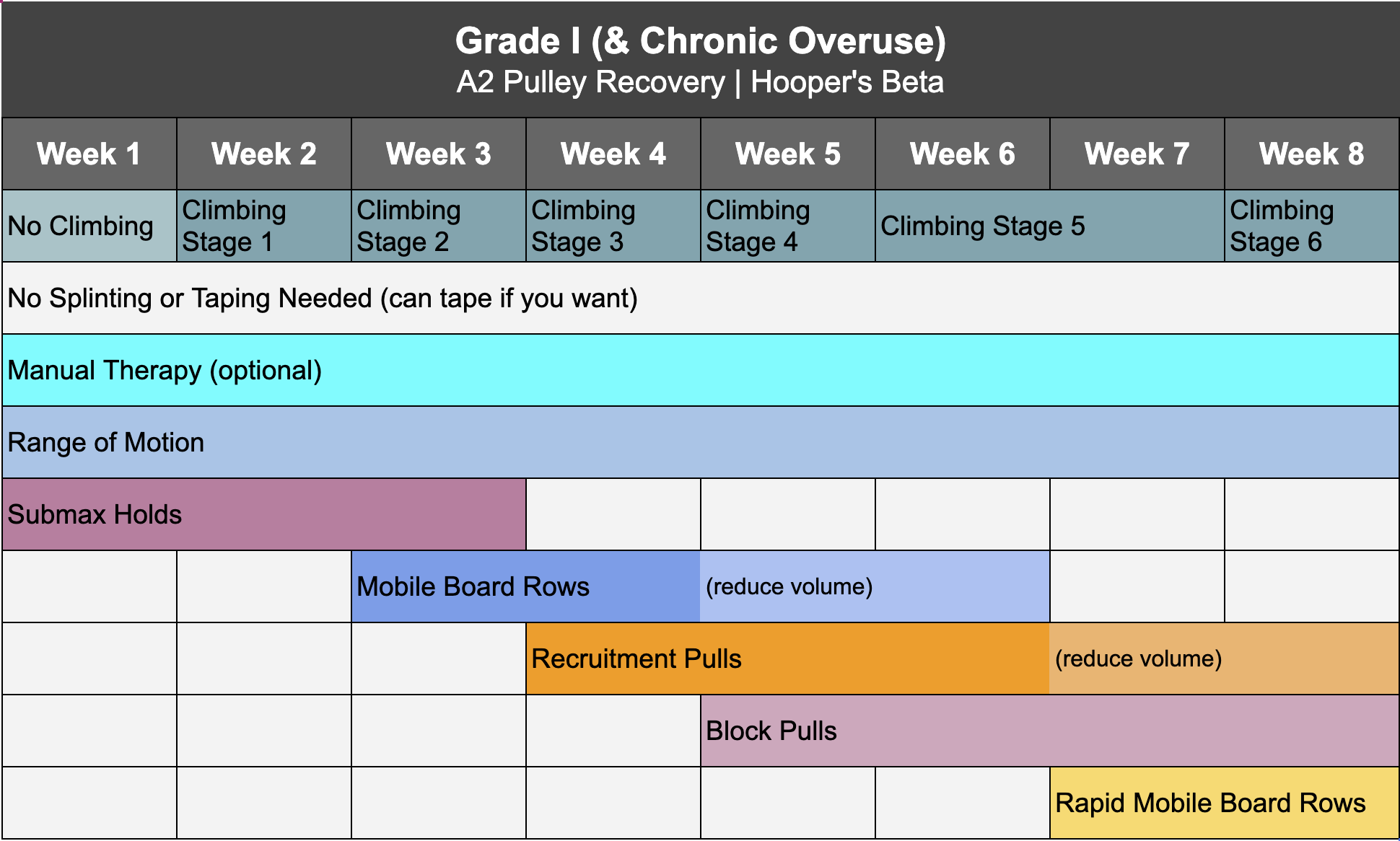
Now to everyone’s favorite part: recovery! Your exact protocol should be determined by your grade of injury, which is why we’ve created separate timelines for grade I, II, III, and IVa. Click here to download the timeline for your specific grade. Note we will not be addressing grade IVb as that requires surgical consultation. For a chronic overuse injury, you can treat it the same as a grade I.
Reminder: if you want to save yourself the trouble of programming all this yourself, you can purchase one of our affordable, proven Recovery Blueprints today on our website at hoopersbeta.com, which has all of the workouts and stages pre-built for you in both a follow-along version, with everything already scheduled, or a self-paced version, where you schedule things yourself based on a recommended timeline.


Deload & Break from Climbing
First thing’s first: for all grades of A2 injury I recommend an immediate break from climbing. Climbing is relatively unpredictable, potentially turning a “small” issue into a much larger one. So, we might as well avoid that possibility. Plus, the brief deload helps us reevaluate any overtraining habits that led us to this point.
For grade I: take 7-10 days off climbing
For grade II: 2 weeks off
For grade III: 6 weeks off
For grade IVa: 8 weeks off
Don’t worry; resting from climbing doesn’t mean stopping all other physical activity (including finger training, which we’ll discuss in a little bit). You’ll just need to make modifications to your activities to ensure you don’t aggravate your injury and exceed 2/10 pain. For grade III injuries especially, be careful to avoid movements that demand excessive grip force, like deadlifts and pullups.
When you do return to climbing, follow this guide (in combination with the grade-specific timeline) to help you determine how much and how hard to climb throughout each stage of recovery.

Splinting & Taping


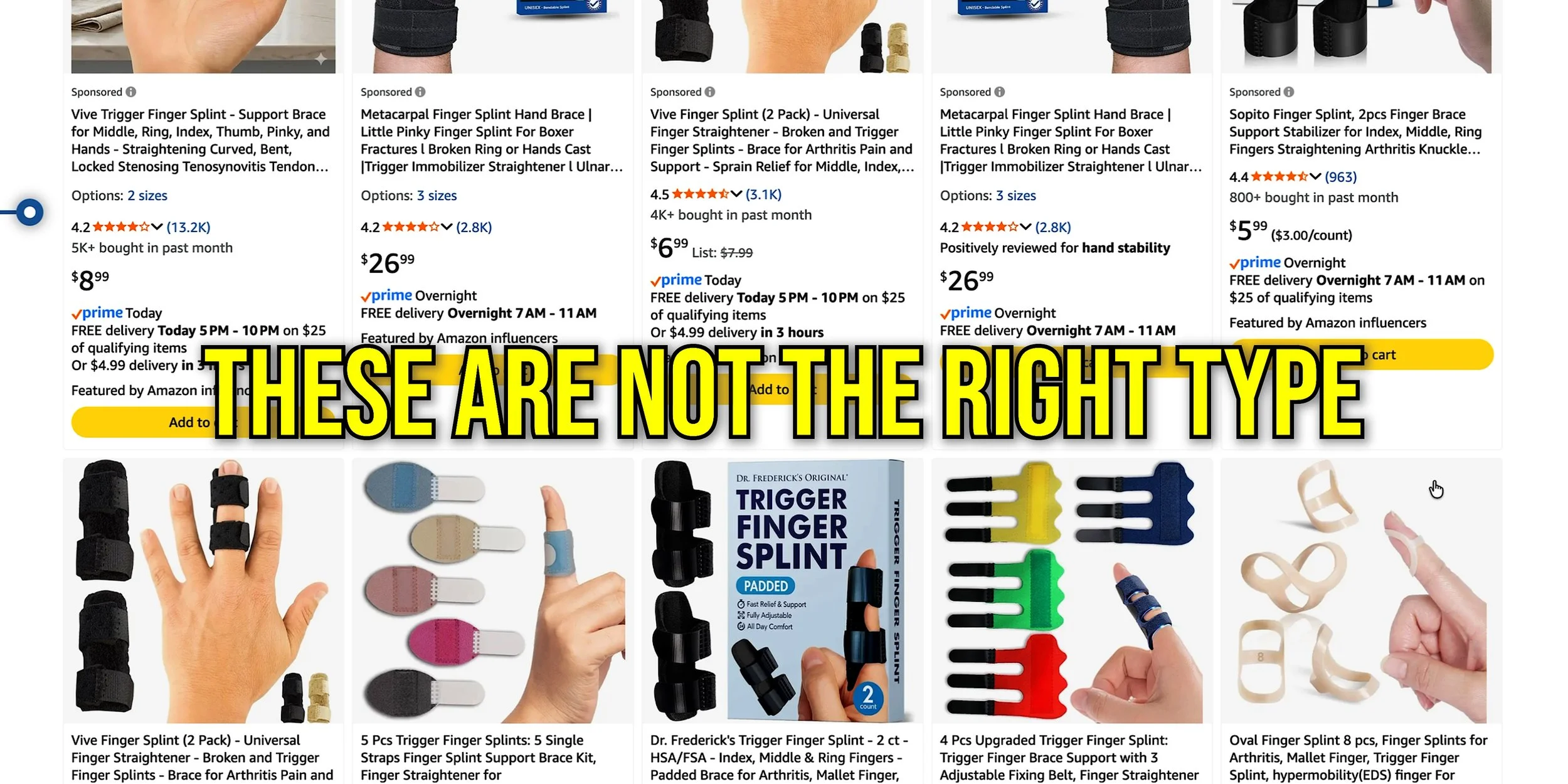
Next, you’ll want to consider supportive taping and/or pulley splinting during your recovery for some grades. The traditional guidelines are as follows:
For grade I, neither is necessary, though taping can be determined by personal preference.
For grade II, supportive H-taping is recommended during any exercise that involves gripping, including finger recovery activities, climbing, deadlifting, pullups etc.
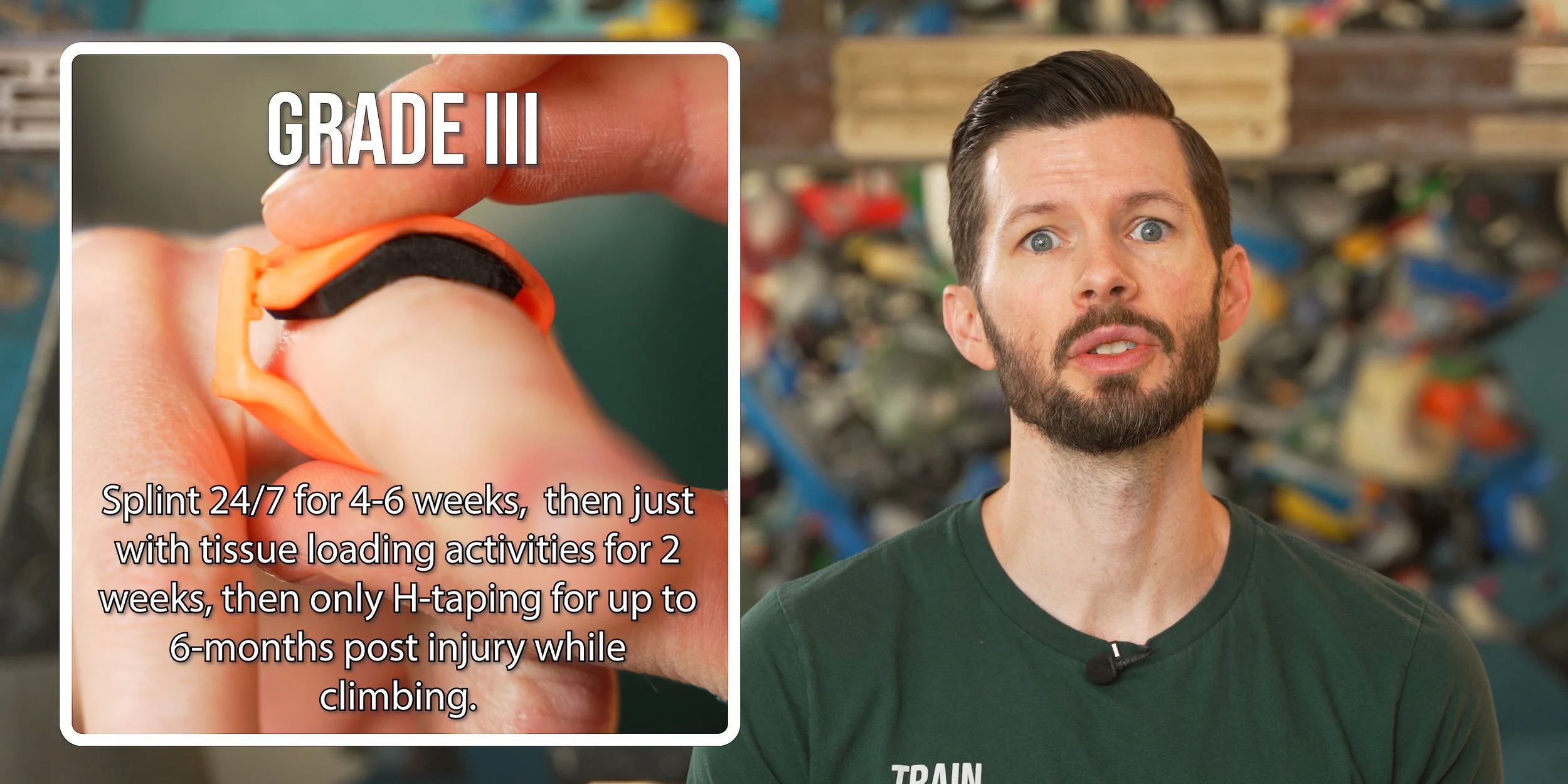
For grade III:
Pulley splint 24/7 for the first 4-6 weeks.
Then, splint only with tissue loading exercises (and any activity involving gripping) for another 2 weeks. For climbing during this time, wearing the splint is optional, but you should be wearing some sort of support while climbing (e.g., h-taping).
Wearing a splint while climbing can be beneficial in that it provides more protection and provides a strong reminder to not overdo it, but it can be a bit cumbersome or uncomfortable, which is why it’s optional.
After that, transition to only h-taping while climbing for up to 6-months post injury.
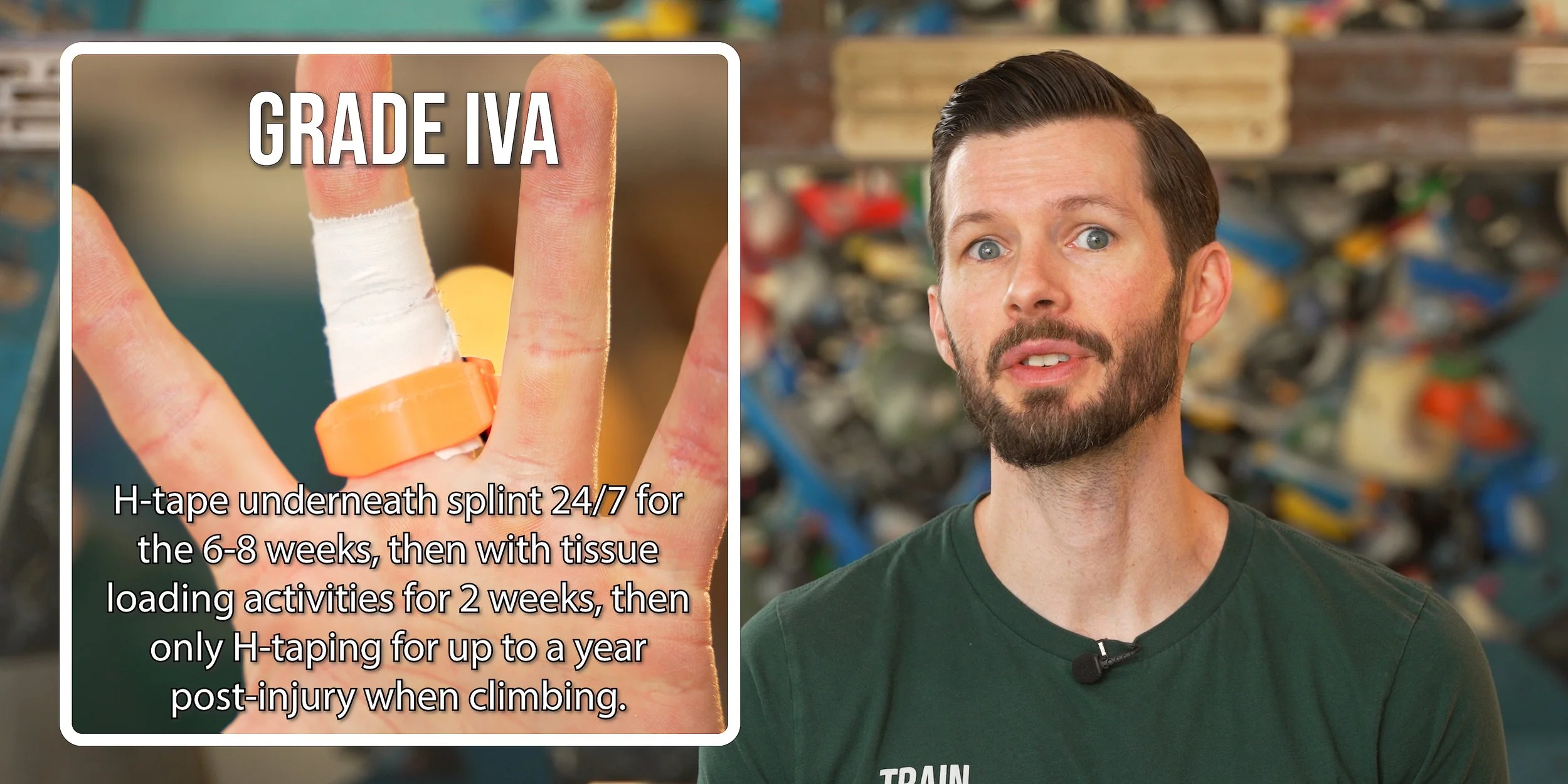
For grade IVa:
Pulley splint + h-taping underneath 24/7 for the first 6-8 weeks.
Then, splint + h-taping only with tissue loading exercises (and any activity involving gripping) for another 2 weeks. For climbing during this time, wearing the splint is optional, but you should be wearing some sort of support while climbing (e.g., h-taping).
Wearing a splint while climbing can be beneficial in that it provides more protection and provides a strong reminder to not overdo it, but it can be a bit cumbersome or uncomfortable, which is why it’s optional.
After that, transition to only h-taping while climbing for up to 1 year post injury.
Note: full finger splinting (immobilization) is not recommended for any of these injuries.
How Tight to Wear the Splint
The pulley splint should be snug enough that it does not move easily on its own, but not so tight that it causes pain or discomfort at rest or during activity.
You should feel some increase in pressure from the support over the pulley when loading the fingers, especially in a crimp position, but there should be only light pressure when at rest.
If you can’t feel any increase in pressure when loading the fingers, it’s too loose.
If you develop bruising or pain on the backside of your finger or feel like blood flow is being restricted, it’s too tight.
Having to adjust the splint tighter and looser throughout recovery is normal. Your finger size may change over the course of a day and over the course of your recovery. It’s OK to adjust or even swap sizes throughout the day as needed.
At night, keep it slightly looser. Our hands tend to swell a bit while we sleep, particularly if they’re recovering from injury, so it’s best to slightly loosen the splint when you go to bed to avoid being awakened by discomfort.




Manual Therapy
Next up: manual therapy (i.e., massage). While research on the efficacy and mechanism of manual therapy is limited, I still recommend it because it’s essentially a zero-risk, potential-gain situation. It costs you nothing and may improve your recovery, as its proposed benefits include tissue remodeling and reorganization, which can be useful across all injury grades.
I typically recommend daily manual therapy for about 3 minutes at an intensity dictated by your current level of irritation/inflammation. The main thing you want to avoid is going too hard or too long and irritating things further, so make sure you keep the pain at or below the usual 2/10 threshold.
Range of Motion
Next up: simple range of motion work. This means fully flexing and extending your fingers in three different positions to encourage blood flow and tissue movement.
To start, touch your fingers to position 1 (at the bottom of your hand). Try to move your fingers in an arc rather than immediately curling them into a fist. Then, fully extend your fingers and repeat for position 2 (in the middle of your hand) and 3 (at the top where you may have palm calluses). Perform about 4-6 reps per position multiple times a day throughout your recovery.
I recommend this range of motion work for all grades, but it can be particularly useful with grade III and IVa to prevent tissue adhesions. Contrary to a lot of recommendations I see, we do not want to immobilize the finger and prevent the tissue from moving with grade I-IVa injuries.
Note: Sometimes, with grade III and IVa, you may not be able to reach position 3 due to range of motion limitations. In that case, you should also work on passive range of motion, where you use your opposite hand to gently encourage greater range of motion than you can achieve actively (without causing more than 2/10 pain, of course).
Off-The-Wall Tissue Loading
The last thing you’ll need to add will of course be off-the-wall tissue loading, which is just a fancy term for specific exercises that help you recover. Loading the tissue is critical for recovery because our bodies need a stimulus to kickstart adaptation (aka healing!). For injury recovery, we choose to get most of this stimulus “off the wall” because it allows us to use consistent low intensities and gradually ramp things up as we heal. At a certain point, the recovery exercises will actually transition into strength training exercises, allowing you to regain, maintain, or even improve your prior level of finger strength.
For grades I and II, I like to start doing this immediately. For grade III, it’s a good idea to wait a few days after the injury, but no more than that. For grade IVa, you’ll want to wait 2 weeks before starting tissue loading.
Submax Holds
Our initial tissue loading activity will be low intensity, high volume submax holds. You’ll simply pull or hang on a 20-35 mm edge (whatever feels comfortable) with one or both hands for 30 seconds, rest for 30 seconds, and repeat.
To help you gauge how hard you should be going with this exercise, use the following guidelines:
Keep the discomfort/pain at or below the usual 2/10 threshold (we don’t want to be causing significant irritation).
Keep intensity low enough that you do not feel fatigued at the start of each rep (about 5-6 RPE).
If you’re doing these on a hangboard, you will likely need to keep your feet on the ground to be able to stay within the intensity guidelines above.
Do about 8-12 reps in total. For grade I-III, perform mostly in a drag but a few in a half crimp. As familiarity and tolerance improves, shift that ratio to about 50/50 drag and crimp. For grade IVa injuries, you’ll need to stick to only the drag position for the first two weeks and then ease into crimps after that.
In the early stages of recovery, perform this twice a day. In later stages, you can reduce to once a day since you should be doing additional tissue loading activities at that point. You can discontinue completely once you start doing recruitment pulls.
As a quick Reminder:
🔥RPE (Rating of Perceived Exertion) is a subjective 1-10 scale that measures the overall feeling of effort and exertion during a set, factoring in muscular fatigue and discomfort. 1 RPE means minimal exertion, while 10 RPE means maximum possible effort (i.e. you took the exercise all the way to failure and could not have handled any more load or reps).
🔋RIR (Reps in Reserve) is a measure of how many more repetitions you could have completed in a set before reaching failure (where your form/velocity significantly drops or pain exceeds 2/10). It's the number of reps you have "left in the tank” at the end of a given set.
Mobile Board Rows
Next, we’ll want to vary our tissue loading tactics with a more dynamic version. We’ll accomplish this by performing band-resisted rows on a comfortable edge. We can modulate the intensity with the thickness of the band, the amount we stretch it, and the speed at which we pull. A band is actually preferred over a cable system here because it starts with minimal resistance and gradually ramps up, making modulating intensity more convenient during early recovery.
To gauge how hard you should be trying, use similar guidelines: discomfort/pain at or below 2/10 and no fatigue at the start of each set. (Notice I said “set” there, not “rep”). About 6-7 RPE.
If you have a force gauge, you can dial these in even further by seeing how hard you’re actually pulling. This is by no means necessary, but it’s another easy way to track your progress over time as it helps you make more informed decisions about your recovery.
I typically recommend 4-6 sets of 10-12 reps in the 6-7 RPE range. For grade I-III, perform half the sets in a drag position and the rest in a half crimp. Once again for grade IVa, you’ll want to start off with mostly drag sets and then ease into crimps over the course of a few weeks. Perform roughly three times per week.
Recruitment Pulls
Next we’ll be progressing our tissue loading with recruitment pulls, which add a beneficial neural-recruitment factor into the mix. This is especially important when recovering from tissue tears because we quite often develop an overactive protective response to loading our injured tissue. Recruitment pulls, coupled with our other training, will help bring that response back to normal levels while also helping to safely retrain our fingers.
To perform recruitment pulls, pick a 20-25 mm edge and a half crimp position and pull over the course of 5-8 seconds, starting at low intensity and gradually increasing within the first few seconds. Rest for a second or two, then repeat.
This style of finger training should feel quite a bit different from the other tissue loading exercises, as all the force should come from trying to curl or press your fingers into the edge rather than simply stopping them from opening up. This is still an isometric exercise, though, so it should not look like a crimp curl. As with the previous exercises, limit your intensity so any discomfort/pain does not exceed 2/10.
I typically recommend about 4 sets of 3 reps, performed roughly three times per week. At first, aim for 6-7 RPE. As you progress, increase to 8 RPE.
Block Pulls
Now, we’ll add block pulls, which are an easily measurable, progressible means of finger strengthening. Block pulls are “yielding isometric” (as opposed to the “overcoming isometric” recruitment pulls), which will help round out our finger recovery.
Block pulls require a mobile board and attachable weights or a cable machine, the most common set up being a loading pin and plates. Simply use a half crimp position to lift the weight off the ground. Do this by straightening your legs rather than pulling with your back or arm. Hold for 1-2 seconds at the top before controlling the weight back down to the ground.
To determine how much weight to use for your working sets, use the following guidelines:
Pain at or below 2/10 (nothing new there).
If you can’t maintain the half crimp for the entire duration of each rep (i.e. your fingers start opening up partway through), you need to reduce the weight.
If you can’t stick within those two parameters for all the recommended reps and sets, you need to reduce the weight.
Stick to 2-3 RIR (reps in reserve). You don’t need to be going to failure with each set.
Don’t forget to progress the difficulty by adding weight over time as your strength improves and pain reduces.
I typically recommend about 2-3 warm up sets of 6-10 reps and then 3-4 working sets of 3-5 reps. These can be performed up to three times per week, but you may need to reduce that frequency depending on how much and how hard you’re climbing at this point. We don’t want to end up “overusing” the tissue and causing disorganized healing in this end stage, so if you’re climbing three times a week you may want to reduce the block pulls to just twice a week (or vice versa).
Rapid Mobile Board Rows
Finally, we'll do a more advanced version of mobile board rows. These will be the same as the previous mobile board rows except that the pulling motion will be executed *as quickly as you comfortably can*. This will help retrain our nervous system and, in particular, our rate of force development (RFD) to get us more accustomed to loading the injured tissue quickly. This can be a huge hurdle for climbers returning from injury as we often become hesitant to commit to dynamic moves. Now that we’re in a later stage of recovery and our pulley is getting stronger, we can perform these rapid rows without risking re-injury.
I recommend you attempt a few pulls at a slower pace and increase the speed over a few reps so you can gauge your comfort level and resistance in the band. If you’re unable to move at a quick pace without causing discomfort/pain, then you should decrease the resistance of the band (even if it feels fine at slower speeds).
Once again, if you have a force gauge, you can measure your force or even rate of force development here, which gives you another useful metric to track over time. For example, if you measure your RFD each session and see that it’s trending up (without increases in pain), you know you’re making killer progress!
I typically recommend 4-6 sets of 8-10 reps at 6-8 RPE, with half the sets in a drag position and the rest in a half crimp. Perform roughly three times per week.
Additional Considerations
Aside from the primary recovery activities, there are a few other things you may be curious about.
Surgery
Surgery is not recommended for an isolated tear of the A2 pulley, even if it’s a complete rupture. It’s usually only considered when multiple pulleys (A2, A3, and A4) have ruptured or if there’s a flap tear as noted earlier.
NSAIDS
Many people wonder whether they can or should take NSAIDs for a pulley injury. Unfortunately, as a physical therapist, I can’t provide specific advice on medication. If you have questions about NSAIDs, I recommend consulting with your physician or pharmacist.
Icing & Contrast Baths
Icing always gets brought up because it can mildly reduce swelling and pain, and contrast baths are said to have similar effects along with increased blood flow. However, I generally don’t recommend either of them for A2 injuries because: they rarely have swelling, the pain is not particularly intense, blood flow can be increased with simple range of motion activities, and neither intervention is all that convenient. You can certainly try them out and see what you think, but don’t let them take away from the most important aspect of your recovery: a well-designed finger loading protocol.
The Most Convenient Way to Recover
If you want to take the guesswork out of your recovery, save yourself a whole lot of time, and get a program that’s specifically designed for your grade of injury, you can get that today on our website at HoopersBeta.com/recoveryblueprint. These are the exact injury-specific programs I’ve used in my practice to help hundreds of climbers get back on the wall pain-free. They’re step-by-step, day-by-day programs guiding you from the earliest stages of healing all the way to regaining full strength and returning to peak performance. Whether you’re dealing with an A2 pulley issue or another finger injury, our Recovery Blueprints are a proven way to fast-track your return to form.
Can I Do Anything to Avoid Pulley Injuries?
It is of course impossible to avoid all injuries, but I think there are some things we should *all* do to help reduce risk.
Avoid repetitive attempts on moves that force your hand open under heavy load. This is believed to be one of the primary mechanisms of pulley injuries in climbers.
Do some form of consistent, measurable grip training to increase work capacity, whether that’s on the wall or off it. You don’t get strong, healthy fingers by just repeating the same old climbing session over and over and hoping your fingers magically stop hurting. Safe progressions are just as key to growth as consistency.
On that note: Train the grips you’re going to use. I often see people only training in a low angle crimp off-the-wall, and then employing high angles on-the-wall. Using our example from before, you should now understand why this can be a major issue.
Warm your fingers up in an appropriate way for the climbing you’re about to do. If you plan on climbing some hard crimps, you should warm your fingers up in the crimp position.
Keep a log, even a basic one, that allows you to get a feel for your long term progress and trends. For example, if your finger strength suddenly starts trending down and you also notice some pain coming on, you now have an early sign that something is off.
Remember to take advantage of that FREE finger injury self-assessment and until next time: train, climb, send, repeat!
DISCLAIMER
The Beta Agency is providing content on its website that aims to inform rock climbing enthusiasts and/or individuals interested in the field of physical therapy of the various physical conditions that may befall those engaged in the sport of rock climbing, for informational purposes only. None of the information provided by The Beta Agency should be regarded as medical advice or construed to be a medical diagnosis of any form. By using our products, services, and/or the information on our website, you acknowledge that you understand this information is not meant to be a substitute for medical advice from an appropriate licensed healthcare professional, and that you will not rely on any of the information you acquire from us as the sole basis, personally or as a suggestion to others, to make any healthcare-related decision(s). If you suspect that you may have a medical condition that you are trying to diagnose, we strongly urge you to seek the advice of an appropriate medical practitioner. If you have a medical emergency, you should contact emergency services immediately.
Click for full Terms and Conditions and Privacy Policy
References
Schöffl V, Hochholzer T, Winkelmann HP, Strecker W. Pulley injuries in rock climbers. Wilderness Environ Med. 2003;14(2):94–100.
Vigouroux L, Quaine F, Labarre-Vila A, Moutet F. Estimation of finger muscle tendon tensions and pulley forces during specific sport-climbing grip techniques. J Biomech. 2006;39(14):2583-2592. doi:10.1016/j.jbiomech.2005.08.027
Schöffl, Isabelle & Baier, Thomas & Schöffl, Volker. (2011). Flap Irritation Phenomenon (FLIP): Etiology of Chronic Tenosynovitis After Finger Pulley Rupture. Journal of applied biomechanics. 27. 291-6. 10.1123/jab.27.4.291.
Walbeehm ET, McGrouther DA. An anatomical study of the mechanical interactions of flexor digitorum superficialis and profundus and the flexor tendon sheath in zone 2. J Hand Surg Br. 1995;20(3):269-280. doi:10.1016/s0266-7681(05)80077-4
Schweizer, A. (2001). Biomechanical properties of the crimp grip position in rock climbers. Journal of Biomechanics, 34(2), 217-223.
Schneeberger, M., & Schweizer, A. (2016). Pulley Ruptures in Rock Climbers: Outcome of Conservative Treatment With the Pulley-Protection Splint—A Retrospective Study of 47 Cases. Wilderness & Environmental Medicine, 27(2), 211-218.
Schöffl, I., Einwag, F., Strecker, W., & Schöffl, V. (2007). Impact of taping after finger flexor tendon pulley ruptures in rock climbers. Journal of Applied Biomechanics, 23(1), 52-62
Schöffl, V., Iruretagoiena, X., Nelson, T., et al. (2024/2025). "Primary Periphyseal Stress Injuries of the Fingers in Adolescent Climbers: A Critical Review."
Iruretagoiena, X., Schöffl, V., Balius, R., & De La Fuente, J. (2023). "High-resolution ultrasound tendon-to-bone distances in partial and complete finger flexor A2 pulley ruptures simulated in human cadaver dissection: toward understanding imaging of partial pulley ruptures." Frontiers in Bioengineering and Biotechnology, 11.
Crowley, T., et al. (2022). "Closed flexor pulley injuries: A literature review and current practice." Journal of Plastic, Reconstructive & Aesthetic Surgery.